ECG Interpretation
ECG Quick Facts
ECG Interpretation
ECG Quick Facts
STEMI Location
100
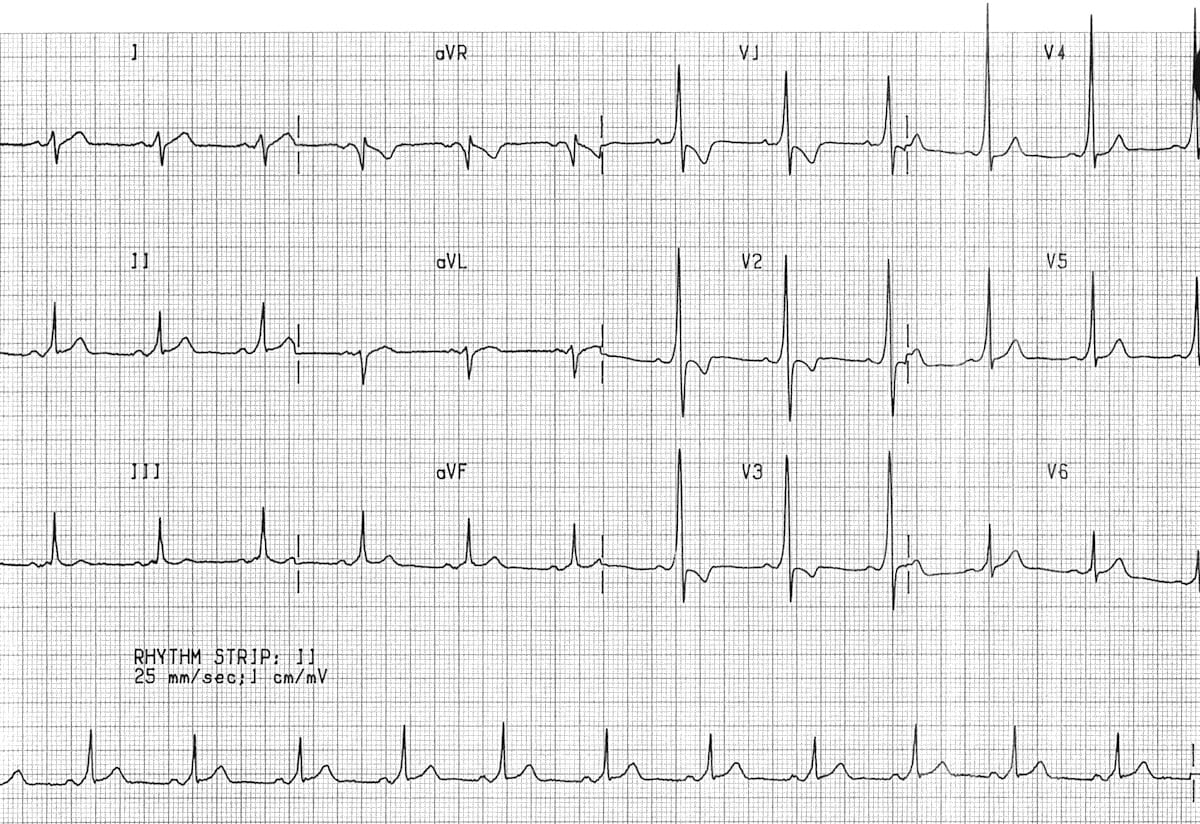
Sinus rhythm ~75bpm with Wolff Parkinson White morphology
100
Describe the electrical conduction pathway of the heart.
Beginning at the sinoatrial node (SA node), conducting through the atria to the atrioventricular node (AV node) through the bundle of His, down the left and right bundle branches and to the purkinjie fibres.
100

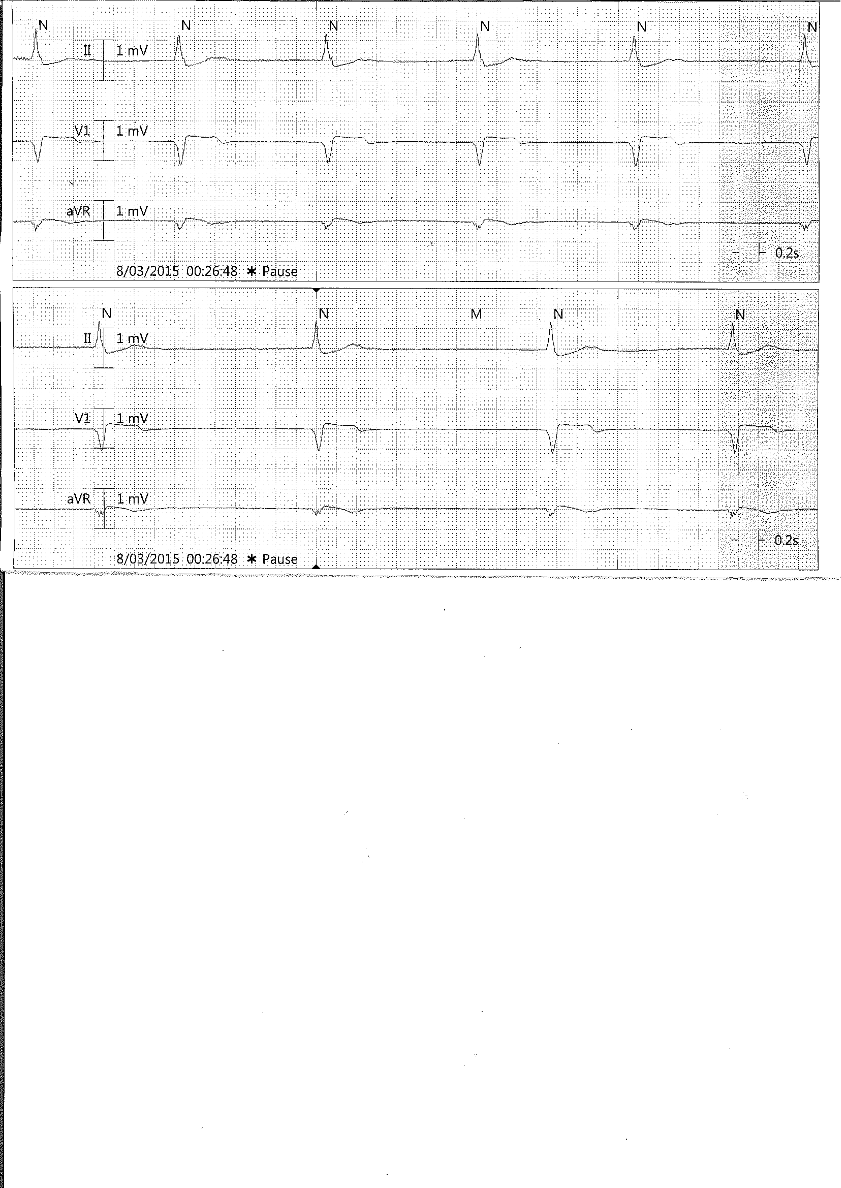
Ventricular standstill
100
What are the rate parameters for sinus bradycardia, sinus rhythm and sinus tachycardia?
Bradycardia <60bpm
NSR 60-100bpm
Sinus tachycardia >100bpm
100

Extensive Anterior STEMI
"Tombstone" morphology STE throughout precordial leads and high lateral leads.
200

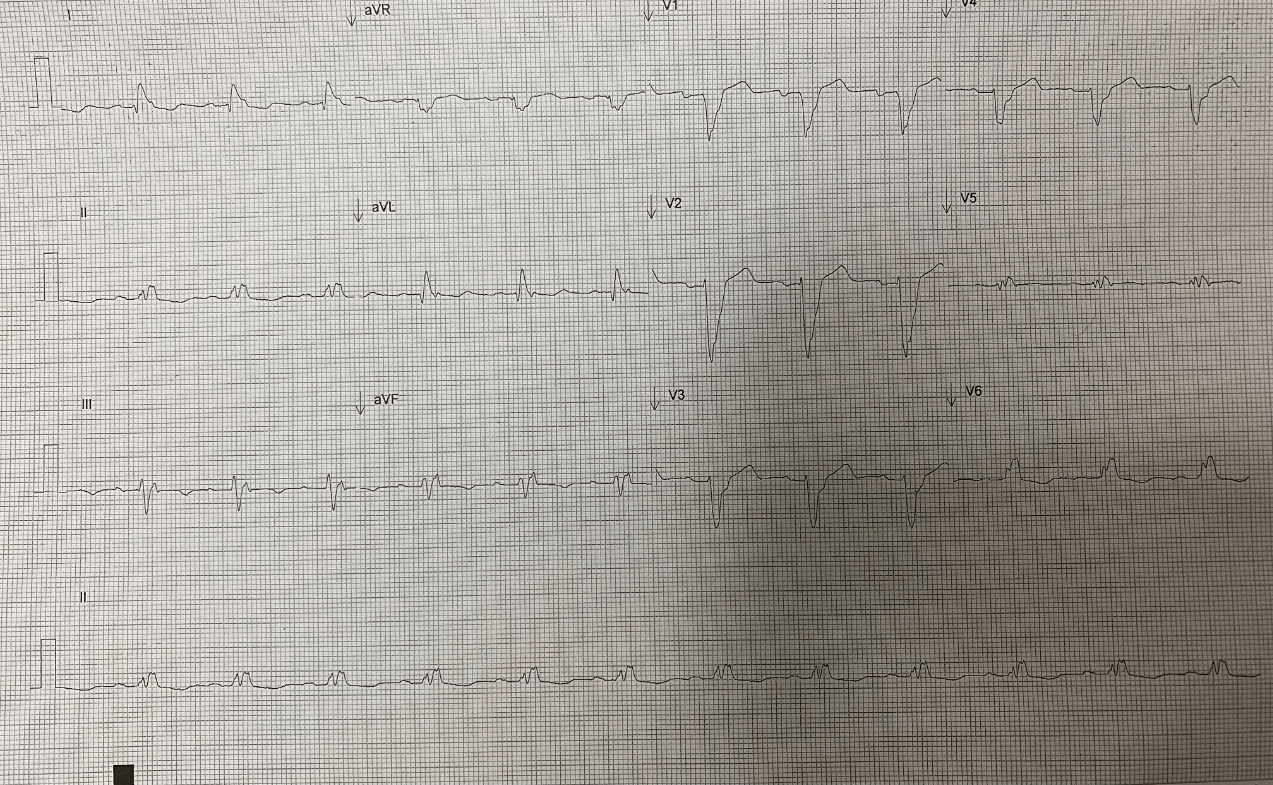
Sinus rhythm with CHB and ventricular escape rhythm at 40bpm.
200
Describe 2nd Degree AV block.
Hint: There is 2
Wenckebach/Mobitz I: progressive lengthening of the PR interval until a non-conducted p-wave occurs.
Mobitz II: intermittent non-conducted P waves WITHOUT progressive prolongation of the PR interval
200
Sinus rhythm 75bpm with LBBB
200
Describe the mechanism of the R on T phenomenon
A PVC occurs during the vulnerable relative refractory period of the preceding cardiac cycle, inducing VF
200

STE in inferior leads, reciprocal changes anterior leads
Inferior infarct
300
Junctional rhythm 38bpm
300
When and Who reported the first ECG?
1903 by Willem Einthoven
300
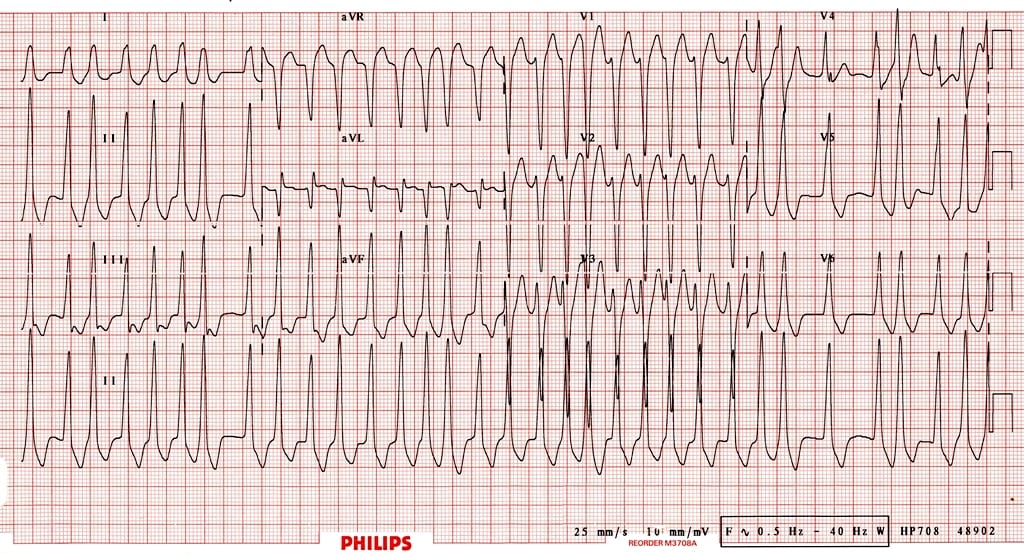
Atrial fibrillation in a patient with WPW (pre-excitation).
Rates up to 300bpm.
300
Explain the clinical significance of a patient with pre-excited atrial fibrillation
The presence of an accessory pathway allows for rapid conduction to the ventricles, bypassing the AV node - rapid ventricular rates may result in degeneration to VT or VF.
300

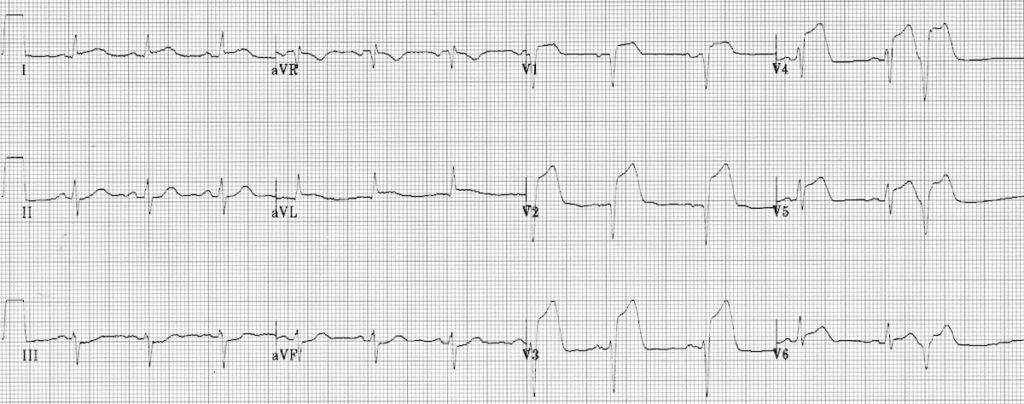
Anterolateral STEMI
STE anterior leads (V2-V4) and lateral leads (1, aVL, V5-6)
Reciprocal STD in inferior leads.
400
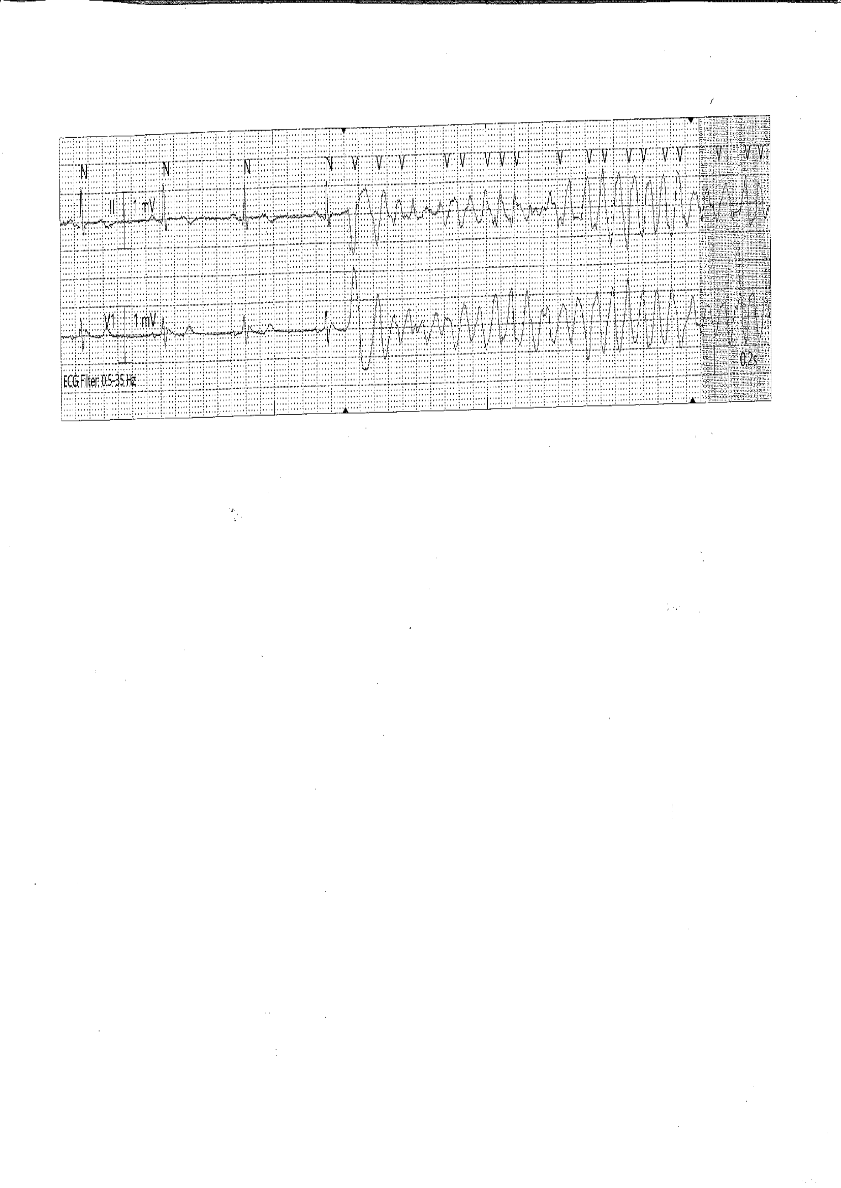
PVC on T wave (R on T) causing Torsades de Pointes
400
Demonstrate and describe the placement of a 12 Lead ECG using correct anatomic terms.

400

Sinus rhythm with AV dissociation.
400
What mechanisms may cause a wide complex during an SVT?
Pre-excitation (accessory pathway)
Rate related bundle branch block
400

Inferior STEMI
Hyper-acute T waves and STE in II, II and aVF
Reciprocal changes in anterior leads.
500
Hint: 18 Y/O presenting with 1/7 chest pain
Sinus rhythm with global STE, STD in V1
Myopericarditis
500
How long is a prolonged QT interval and what arrhythmia are people with a long QT at risk of developing?
Prolonged if >440ms in men and >460ms in women. Torsades de pointes.
500

Atrial fibrillation with RBBB, 92bpm
500
Describe the regions of an ECG in relation to localising acute coronary syndrome.

500

Inferolateral STEMI
STE in inferior (II, III and aVF) and lateral (I, V5-6)
STD in V1-V3 suggesting posterior extension.
600

Artifact
600
What ECG findings would you see associated with sinus node dysfunction?
Hint: there is 8
Sinus bradycardia
Sinus arrhythmia
Sinus pause or arrest
Sino-atrial exit block
Chronotropic incompetence
Tachy/brady syndrome
Wandering Atrial Pacemaker
Atrial fibrillation
600

Monomorphic VT, shock on T wave causing VF, shock reverting to sinus rhythm.
600
What is the lead on the top right of Einthoven's triangle?
Right arm
600
Anterior STEMI
STE V1-6
Reciprocal changes III and aVF