Splints!
~Crazy Kids~
Ortho Emergencies
FALLS
Miscellaneous :)
100
What exam must be performed and documented before and after every splint application?
NEUROVASCULAR EXAM?
- Check and document: pulses, capillary refill, and sensation on the affected and contralateral side
https://www.aliem.com/splinter-series-splint-application-principles-102/
100
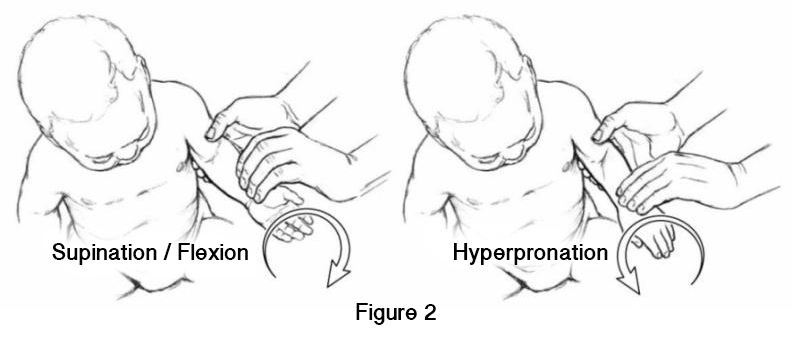
What are the two methods of reducing a Nursemaid's elbow (Radial Head Subluxation)?
1. Hyperpronation - apply pressure to radial head in a medial direction and use your opposite hand grasp the distal forearm and hyperpronate the arm. +/- flexion at the time of maximal hyperpronation.
2. Supination/Flexion - also apply pressure to radial head and use opposite hand to supinate the forearm and then flex the elbow past 90 degrees in one smooth motion.
100
A 32-year-old woman presents to the ED with severe right leg pain after falling down a flight of stairs. On exam, her right lower leg is swollen, exquisitely tender, and firm to the touch. Dorsalis pedis and posterior tibial pulses are faint but present. An x-ray is shown. This is worrisome for which surgical emergency?

Acute Compartment Syndrome
- increased intramuscular pressures and impaired circulation within a closed compartment, commonly associated with traumatic injuries. The anterior tibial compartment of the lower leg is the most common location. If left untreated, it can lead to irreversible muscle necrosis and nerve damage. Diagnosed by measuring compartment pressures. Treated with fasciotomy.
100
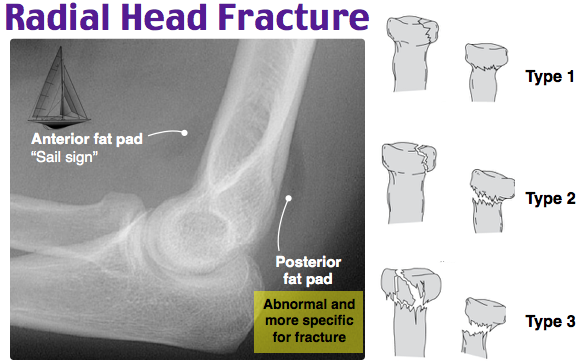
Which of the following is indicative of a radial head fracture?
- A) Displacement of the radiocapitellar line
- B) Posterior fat pad sign
- C) Pronator sign
- D) Wrist drop
B) Posterior Fat Pad Sign
100
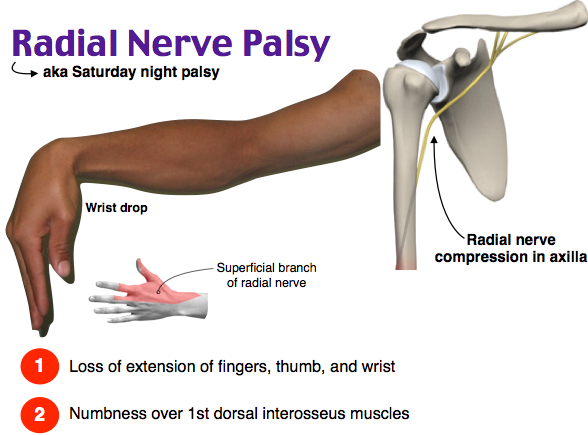
A patient presents to the emergency department with wrist and hand weakness. He is holding his wrist in flexion and his hand is hanging limply. He is unable to extend his wrist against resistance. Which of the following nerves is most likely injured?
Radial Nerve/“Saturday night palsy”
- The patient has wrist drop, which is caused by injury to the radial nerve (innervates the dorsal extrinsic muscles in the forearm, which function in wrist and MCP extension, as well as abduction/ extension of the thumb.)
200
What is the recommended splint for a SCAPHOID, TRAPEZIUM, or LUNATE fracture?

200
Which Salter-Harris Type involves the physis and epiphysis?
Salter-Harris Type III


200
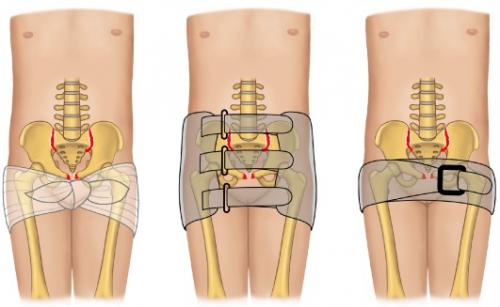
A 42-year-old farmer presents by ambulance after being pinned against a wall by a tractor. His vitals are 95/60, HR 125, RR 18, O2 98% RA. He is pale, diaphoretic, and complaining of severe pain in his hips and groin. FAST negative. Pelvis Xray as follows. What is the most appropriate next step?

Pelvic Binder/Wrap Pelvis Across Trochanters
Hemorrhagic Shock secondary to open-book pelvic fracture. Be sure to exclude other sites of hemorrhage! Wrapping the pelvis helps to minimize the size of an expanding pelvic hematoma by reducing the size of the pelvis and helping to tamponade the disrupted vessels.
200
What injury is associated with a high riding patella (patella alta) and is likely to cause the inability to actively extend at the knee?
Patellar Tendon Rupture

200
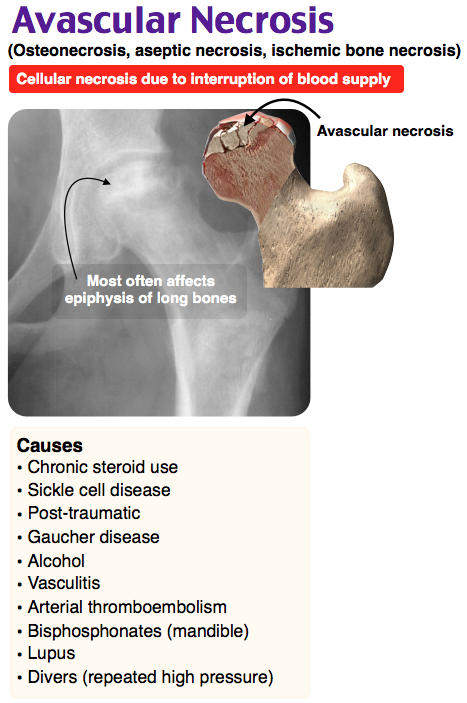
A 33-year-old man with a history of sickle cell disease presents with progressive hip pain with ambulation. His vital and labs are within normal limits. A hip xray is seen below. Which of the following is the best management of this patient?
- A) Emergency surgery
- B) Hydromorphone, IV fluids, and discharge with crutches and follow-up
- C) MRI of the hip and administration of piperacillin-tazobactam and vancomycin
- D) Proper analgesia, sedation, and hip reduction

B) Hydromorphone, IV fluids, and discharge with crutches and follow-up
AVASCULAR NECROSIS: occurs when the blood supply is affected to a bone, such as when sickled cells form in sickle cell disease and occlude the vasculature. It can be asymptomatic and discovered incidentally or can present with pain in the affected joint that is exacerbated by weight bearing that slowly increases as the disease worsens.
Conservative measures can be tried typically for four to six months --> if symptoms are refractory or worsening, it will be treated surgically via core decompression and, if that fails, arthroplasty.
300
What is the recommended splint for a SUPRACONDYLAR fracture?


300
A 7-year-old boy with a history of cognitive delay presents to the Emergency Department with his parents for arm pain. His parents do not remember any trauma to the patient's arm. They report he was running around and began crying. The X-ray of his arm is above. What is the diagnosis and what is the most appropriate next step in management?
GREENSTICK FRACTURE - Place sugar-tong splint and follow-up in orthopedics in 1 week. (** if >10' angulation, should be seen by orthopedist in ED, may require completion of fracture for proper anatomic reduction)
Most commonly seen when a child lands on their arm. Children's bones are more pliable than adults, which allows for the bone to bow instead of break - one side of the cortex is fractured while the other side compresses.

300
A 73-year-old man with a history of arthritis presents with fever, severe right knee pain x 3 days with inability to bear weight since this morning. Exam with exquisite right knee tenderenss and large effusion. Arthrocentesis with turbid fluid; lab analysis reveals the following: WBC 55k 95% neutrophils and glucose 60mg/dL, gram stain and crystal analysis pending. What is the likely diagnosis?
Septic Arthritis
Most commonly caused by staph aureus in adults. Risk factors include elderly age, prosthetic joints, IV drug use, immunocompromise. Knee is most commonly affected. Will require admission and orthopedics consult for joint irrigation.
300
A 16-year-old girl fell while skiing and presents with right thumb pain. Exam reveals tenderness and swelling of right thumb. X-ray negative. Valgus stress at the MCP results in increased pain and deviation of 40 degress. What is the treatment?
Thumb Spica and urgent referral for surgical management.
Skier's Thumb (Gamekeeper's Thumb) = rupture of ulnar collateral ligament
* Partial tears typically recover with immobilization, whereas complete ruptures invariably need surgical repair.

300
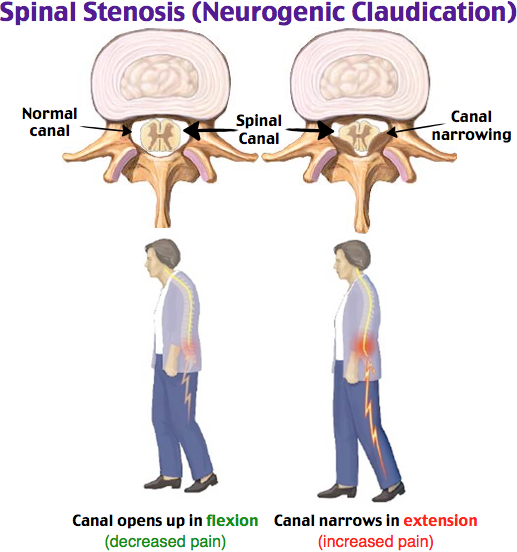
A 67-year-old man presents to the emergency department with lower back pain that has been gradually worsening x 1 month. Associated with burning lower extremity pain, and numbness whenever he is walking or working. Symptoms improve when he is cycling or pushing a grocery cart. Physical exam reveals no weakness, no loss of sensation, and a stable gait. There is no tenderness to palpation of the midline spine or lateral to the spine. What is the most likely diagnosis?
Neurogenic claudication (spinal stenosis):
- Narrowing of the spinal canal compresses the spinal cord, causing lower back pain that may radiate to BLEs +/- paresthesias. Symptoms improve with leaning forward (opens up the spinal canal/reduces spinal cord compression). The diagnosis is confirmed with an outpatient spine MRI. Treat with PT; if refractory, may involve surgical decompression.
400
What are THREE reasons NOT to splint immediately in the ED?
- Open fracture: will require operative irrigation and debridement before appropriate reduction and splinting.
- Concern for compartment syndrome or acute neurovascular compromise: the pressure of splint can worsen vascular compromise and necrosis.
- Chronic neuropathy or complex regional pain syndrome: increased risk for pressure ulceration
- Evidence of infection: splint can create a nidus for infection and covers the area
https://www.aliem.com/splinter-series-splint-principles-101/
400

A 3-month-old girl born at term via cesarean section due to breech position presents to the emergency department after her mother felt a pop in her left leg while changing her diaper. She appears well. She has no instability on the Ortolani and Barlow maneuvers but her left hip has limited abduction compared to the right and she has the above skin findings. Which of the following is the best next test recommended to confirm the diagnosis in this patient?
- A) Galeazzi sign
- B) Hip ultrasound
- C) Pelvis MRI
- D) Pelvis X-ray
B) Hip Ultrasound
Developmental dysplasia of the hip (DDH) is common in infants born in breech position, and long-term outcomes are improved with early diagnosis and treatment. Infants with DDH have only partial to no contact between the acetabulum and femur due to abnormal development and physiologic joint laxity and often leads to avascular necrosis. This laxity is usually suspected with the Ortolani and Barlow maneuvers in young infants. At about 3 months, the most reliable physical exam finding of developmental dysplasia of the hip is a limitation in abduction. Asymmetric skin folds, also suggest DDH but are common in infants with physiologically normal hips and are not present when the DDH is bilateral. Before 4 to 6 months of age, the diagnosis of DDH is best made by a hip ultrasound due to the head of the femur being completely cartilaginous.
Treatment of DDH:
- < 6 months: Pavlik harness.
- ≥ 6 months: closed reduction under general anesthesia in the OR
400
A 25-year-old man presents with right hip pain after MVC. Right leg is shortened, adducted, and internally rotated. He has decreased sensation of the posterolateral leg and weakness with dorsiflexion of the foot. His hip x-rays are as follows. Which nerve is most likely affected?

Sciatic
- Posterior Hip Dislocation, most commonly from dashboard injury from MVC. May cause sciatic nerve palsy, femoral nerve palsy (more common), or femoral artery injury. Orthopedic emergency for closed reduction, risk of avascular necrosis of femoral head increases in direct proportion to delay in reduction.

400
21-year-old track-and-field athlete trips during her race resulting in severe foot pain. She presents with erythema and edema. During examination, stabilization of the calcaneus and rotation of the forefoot results in a clicking sensation and severe dorsal foot discomfort. Toe flexion and extension is maintained in a normal, nonpainful range. You most likely suspect a dislocation of which of the following joints?
- A) Fibulotalar
- B) Metatarsophalangeal
- C) Tarsometatarsal
- D) Tibiotalar
C) Tarsometatarsal (Lisfranc Injury)
Fracture-dislocation of the tarsometatarsal joints is commonly called a Lisfranc injury. These joints exist between the three cuneiforms and the cuboid proximally and the five metatarsals distally, with the key joint being the “locking” interaction between the middle cuneiform and the second metatarsal base. Common mechanisms of injury include trauma and tripping. Pain is located on the dorsum of the midfoot, as compared to perimalleolar ligamentous pain. As such, Lisfranc injuries are easily misdiagnosed as ankle sprains. A key exam finding is pain with forefoot rotation against a stabilized hindfoot (calcaneus). This maneuver is not painful in ankle sprains or ankle mortise injury, but severely painful with Lisfranc injuries. Diagnosis can be upheld when an AP radiograph reveals lateral shift of the second metatarsal off the middle cuneiform. Nondisplaced injuries are treated with non-weight bearing and casting, however, any displacement necessitates surgical intervention.

400
What are Kanavel's signs? What are they signs of?
Kanavel's Signs of Flexor Tenosynovitis
exquisite tenderness over the flexor tendon;
the finger sits in a resting flexion;
pain on passive extension of the finger (more marked at the proximal end);
fusiform swelling of the whole finger.
*Requires urgent hand referral

https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6532803/
500
What are TWO of the indications for a POSTERIOR SHORT LEG SPLINT?
Any two of the following: ankle sprains, talus, calcaneus, navicular, cuboid, cuneiform, metatarsal, Lisfranc fractures (tarsometatarsal), isolated fractures of the fibular or tibia?

500
A 13-year-old patient presents to the ED after a twisting knee injury while playing soccer. There was a pop, and the patient was subsequently unable to bear weight due to pain and knee instability. The swelling and pain increased in the hours after the injury occurred. On examination, there is a large knee effusion and a positive Lachman test.
What is your suspected diagnosis (*there are TWO things wrong)?

Anterior tibial spine avulsion fracture with ACL injury.
- Anterior tibial spine is the insertion point of the ACL. more common in peds --> fractures can be caused by a twisting or pivoting knee injury, hyperextension, or direct trauma, with or without concomitant ACL injury.
BONUS: What is your management and disposition? Long leg knee immobilizer locked in full extension and orthopedics referral within 1 week.
- Pearl: In contrast to a typical ACL rupture, which can be treated with or without surgery and can wait a few weeks for a follow-up, these injuries should have a more urgent surgical evaluation and generally need operative repair
 https://www.aliem.com/splinter-series-dont-forget-tibial-spine/
https://www.aliem.com/splinter-series-dont-forget-tibial-spine/
500
You suspect necrotizing fascitis. Which antibiotic do you want to start first and why?
Clindamycin (600-900 mg IV q8h) - immediately shuts down toxin production!
Regimen must cover: gram positives and negatives, anaerobes, generally MRSA coverage
- Type I: polymicrobial; Type II: GAS; Type III: gas producing/clostridium
- Piperacillin-Tazobactam 3.375-4.5g q6hr AND clindamycin 600-900mg q8hr AND vancomycin 1gm IV q12hr (consider weight base 20 mg/kg)
- Piperacillin-Tazobactam 3.375-4.5g q6hr and linezolid 600mg q12hr is an alternative regimen
- Linezolid was found to be generally superior to vancomycin in soft tissue infections
- Meropenem if history of resistant gram-negatives or nosocomial risk factors
- In diabetics, maintain strict glycemic control
- Surgical exploration and debridement
500
A 42-year-old woman presents to the emergency department with left wrist pain. She slipped and fell on the ice, falling forward onto her left hand. Her wrist radiograph is shown above. What is the diagnosis?

Perilunate dislocation (Stage II Carpal Ligamentous Injury)

Class of carpal ligamentous injuries:
1. Stage I injury: scapholunate dissociation = widening of the scapholunate joint on PA radiograph, dubbed the “Terry Thomas sign”
2. Stage II injury: Perilunate dislocation, is best seen on the lateral radiograph of the wrist, showing the capitate bone dislocated and dorsally displaced relative to the lunate. The lunate maintains its articular connection to the radius, distinguishing it from a lunate dislocation. The PA view shows an overlap of the carpal rows. The most common mechanism is a FOOSH. Pain, swelling, and tenderness are noted over the dorsum of the wrist, particularly in the region of the scapholunate ligament. Patients with suspected perilunate dislocation require emergent orthopedic consultation for open fracture reduction and stabilization. Complications include median nerve compression and avascular necrosis.
3. Stage III similar to perilunate dislocation but includes dislocation of the triquetrum.
4. Stage IV injury: lunate dislocation, involves rotation of the lunate in a volar direction, with a “spilled teacup sign” of the dislocated lunate on lateral radiographs or the “piece of pie sign” referring to the triangular appearance of the displaced lunate on PA radiographs.
**ALSO: Recall that patients with anatomical snuffbox tenderness should have ortho follow-up for further imaging to re-evaluate for fracture and avascular necrosis.
500
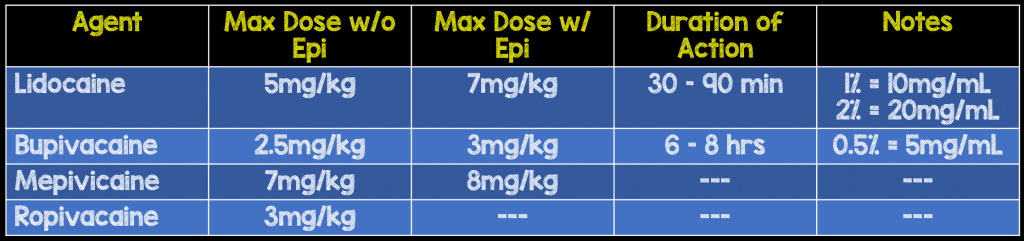
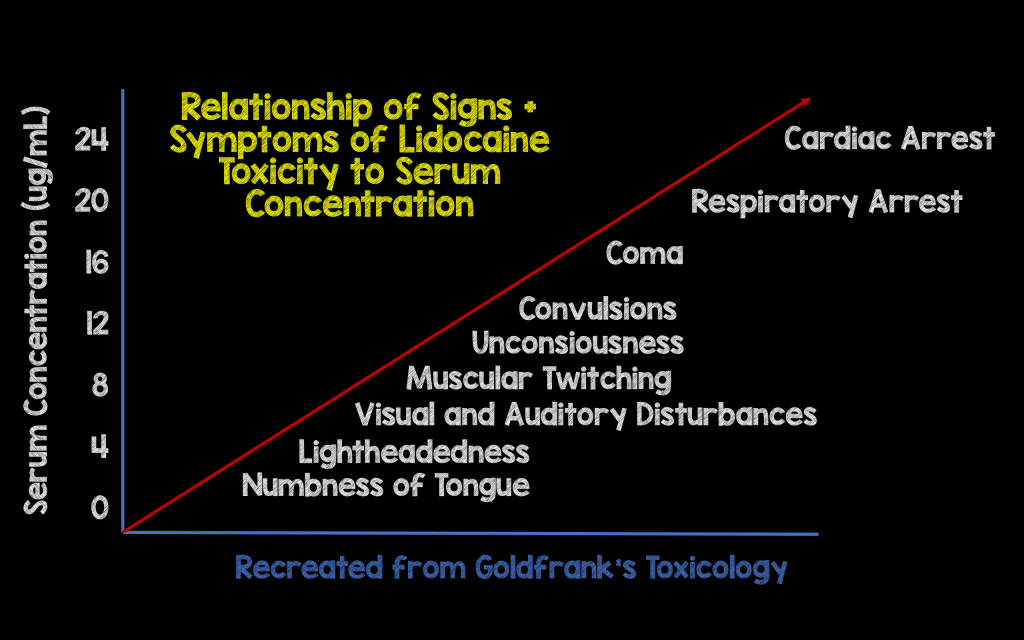
You're doing a nerve block. What is the maximum amount (in mg/kg) of Lidocaine without Epinephrine you may give to avoid local anesthetic systemic toxicity?