Respiratory
Colic
Lameness
Clinical Skills
General PE
100
What can you do to better hear the lung sounds in a horse?
rebreathing test
100
From dorsal to ventral, describe the anatomy of the GIT tracT on the left and right side of the body.
right: cecum, right dorsal colon, left dorsal colon
Left: Descending colon, Jejunum, left dorsal colon, left ventrall colon
100
How would you target you PE around a MSK case?
1. Cardiovascular system (especially digital pulses)
2. MSK exam (palpate every joint and bone for inflammation, swelling, ect, examine hoof)
3. Gait analysis
4. Auscultation heart and lungs
100
What are the three sites for IM injections?
1. Triangular area in the neck: Dorsal border (crest of neck Ventral to nuchal ligament), caudal border (scapula), ventral border (cervical vertebrae)
2. Pectoral muscles
3. Caudal thigh muscles (either semitendinosis or membranosis)
100
What is the first part of a PE?
OBSERVE!!!
1. Mentation/ temperament
2. Appetite
3. respiratory rate/effort
4. Behavioral changes (flank watching/ pawing)
5. Manure
6. BCS
7. Environment
8. Posture, stance, and conformation
200
A 8 year old QH presents to you with clinical signs indicating a respiratory issue. Describe what parts of the PE you would focus on To make this a respiratory targeted exam?
1. Respiratory system (nose, trachea, thoracic lung sounds, etc.)—-> possibly include maxillary sinus and guttural pouch which are air filled structures not directly related to the respiratory system
2. CV system (mm for perfusion and hydration status, heart sounds, pulses —>digital, facial, transverse facial)
3. Systemic (lymph nodes)
4. Overall symmetry of the horse (face, body, etc)
Consider GI exam If horse is dyspneic. Colic doesn’t directly cause respiratory disease but may lead to abnormal breathing.
200
Besides the 4 quadrants on the left and right side of the horse, where else can you listen when assessing a colic?
listen to the ventral abdomen for possible sand impaction. Would sound like waves crashing on a beach.
200
Name 3 differentials for a lame horse?
1. Laminitis ( grain overload, SIRS, PHF, etc.)
2. Trauma/ fracture
3. Hoof abcess
4. Septic joint
5. Soft tissue injury (tendons)
6. Mechanical overload
200
Describe how to give an IM injection at each site
1. Caudal thigh muscles ——> stand on opposite side of the muscle that you are injecting, inject either the semitendinosis or semimembrinosis to the hub of the needle, aspirate and inject
2. Pectorals—> grab the muscle with your thumb and forefinger in each of the grooves. Stick needle in perpendicular to the hub, aspirate ton check for blood, and inject. This area is most likely to swell so not used as much.
3. Neck—-> pinch skin to desensitize area. Slide needle to hub, aspirate, and press plunger and administer vaccine.
Use an 18g or 20g needle
200
What is the TPR of the horse?
T: 99-101.5
P: 26-48
R: 8-16
300
Name at least 3 differentials for a horse with respiratory signs?
1. Degenerative
——-> laryngeal hemiplegia
2. Anomaly/ autoimmune
——-> nasal polyps
3. Metabolic/ mechanical
4. Neoplasia
—-> lung masses?
5. Inflammatory, infectious, iatrogenic, idiopathic
—> EHV-1, EHV-4, equine influenza, African horse sickness, equine adenovirus, equine arthritis, EHV-5
—-> EQUINE Multinodular pulmonary fibrosis (mature horses),
—-> parasits, fungal infections (aspergillosis, guttural punch mycosis)
—> equine asthma
6. Trauma/ toxic
——> exercise induced pulmonary hemorrhage
7. Vascular
300
A horse is being referred to you for potential colic signs. Describe what systems you would focus on to make this a targeted exam.
1. GIT (mouth, esophagus, gut sounds)
2. Respiratory (auscultate lung sounds)
3. Cardiovascular system (mm, CRT, auscultation of the heart)
4. Rectal exam
300
Describe how to give A SQ injection.
Subcutaneous injection is rarely performed when working with horses.
Medications delivered subcutaneously must be labelled for that route; they must be sterile and non-irritating to the tissue. If used, choose the lateral neck for SQ injection.
300
Where should you listen to cecal flushes in the horse? How many should you hear?
right paralumbar fossa. 2-3 flushes per minute
400
potential diagnostics for narrowing down your differentials?
1. Obtain full history and any additional info (ex: is respiratory issue at work or rest?)
2. determine if it is upper or lower airway.
3. Endoscopy
4. Trachea wash
5. Imaging
400
What are 3 differentials for a colic. How do you determine if it is strangulation vs intralumenal?
1. Strangulation (pain may be more severe), may develop reflux
—-> strangulating lipoma (older horses)
—-> nephrosplenic entrapment/ left dorsal displacement of the large colon ( moderate colic, TPR N- slightly high, US can’t visualize Left kidney, may be reflux, belly tap normal),
—-> small intestinal strangulation
2. Intraluminal (Pain may be moderate)
—-> ileus secondary to bacterial enteritis
—-> spasmodic colic/gas colic (no reflux, typical PE findings usually normal or slightly increased/decreased, increased GI sounds)
—-> impaction colic (if pelvic flexors impaction may have decreased fecal output with dry feces, sought dehydration, and normal to decreased GI sounds), (small colonimpaction—> similar to pelvic flexure, moderate pain, abdominal distention, consider breed and history e.g mini horse/pony, foreign body ingestion) (cecal impaction can have mild to severe pain, decreased fecal output, decreased GI sounds, often not displayed until cecal impaction is severe, risk of rupture) (sand impaction “ocean waves)
—> slow GI transit—-> mucous in feces
400
Describe how to give an IV injection to a horse?
1. Draw up the medication to be given into an appropriate size syringe, using sterile
technique.
2. Use your non-dominant hand to hold off the vein within the jugular groove at about
the midpoint of the neck. Your goal is to enter the jugular vein in the cranial 1/3 of
the neck, where the risk of accidental carotid artery injection is minimized.
3. Take time to clearly identify the jugular vein; note its position within the jugular
groove and visualize its trajectory.
4. Hold an 18 gauge needle between your thumb and index finger, with the bevel facing
outward.
5. Using a 20-30 degree angle, penetrate the skin and enter the jugular vein with
confident intention.
a. An excessively shallow angle may result in SQ placement of the needle.
b. Use of an angle greater than 30 degrees risks inadvertently going through the
vein to end up in the carotid artery.
c. Thread the 18 gauge needle into the vein all the way to the hub.
d. If the vein is missed, try to withdraw partially and redirect without removing the
needle from the skin.
6. Attach the syringe to the properly placed needle, aspirate to verify continued correct
placement within the lumen of the vein, and inject. *If the horse jumps around be
sure to stop injecting! Movement of the head and neck may force the needle into
the carotid artery.
400
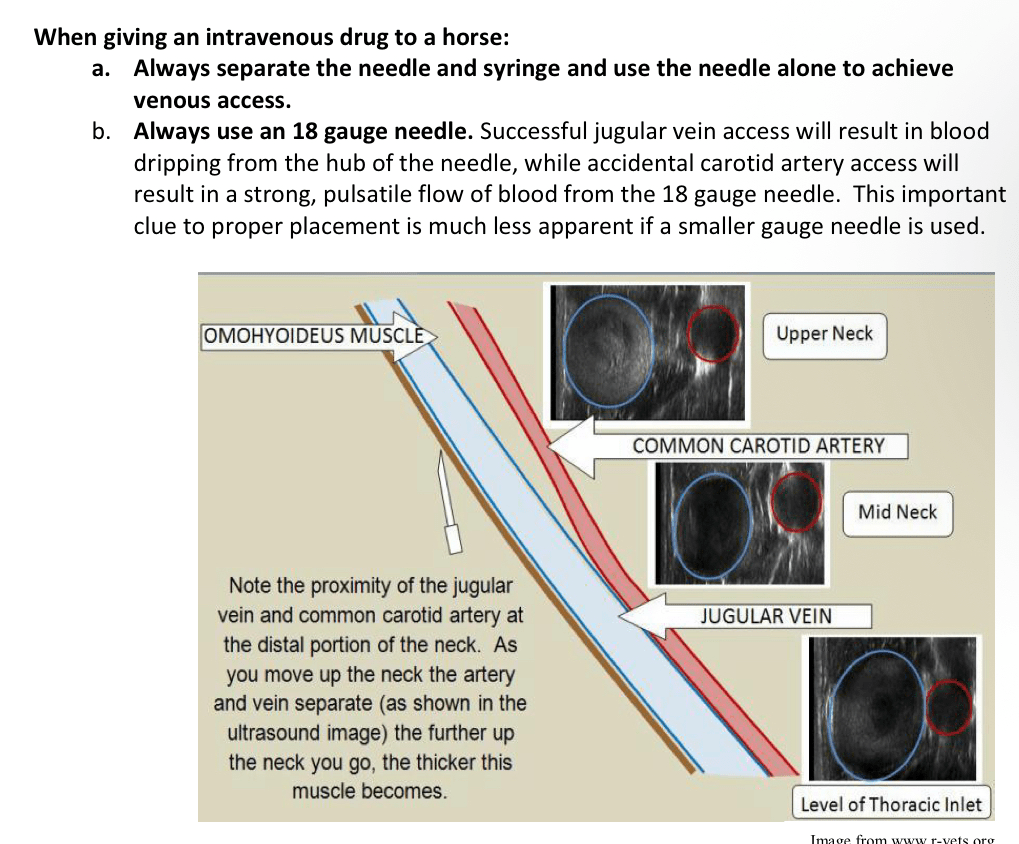
What would you expect to see in the jugular groove of the distal 3rd of the neck and why?
You should see consistent pulsation due to the carotid artery being just deep to the jugular vein. Additionally, it is very close to where it empties in the right atrium, so every time the atrium contracts you will see a pulsation And slight distention. BONUS: if you saw bounding pulsation in the cranial 1/3, then this is an indication that sometime in the CVS is abnormal.
500
Describe venipuncture
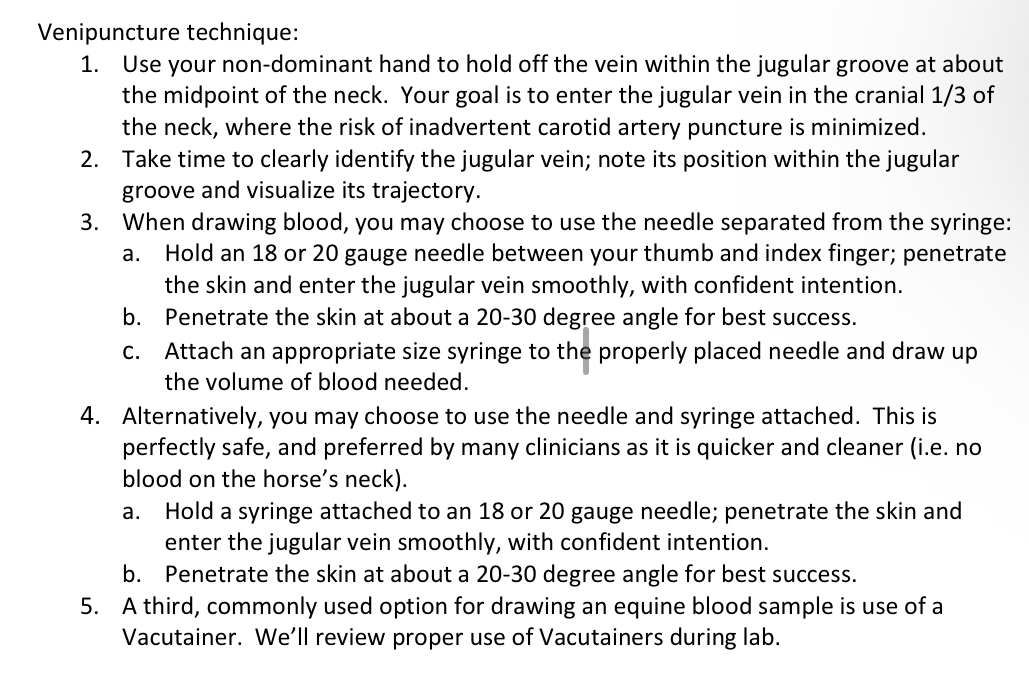
500
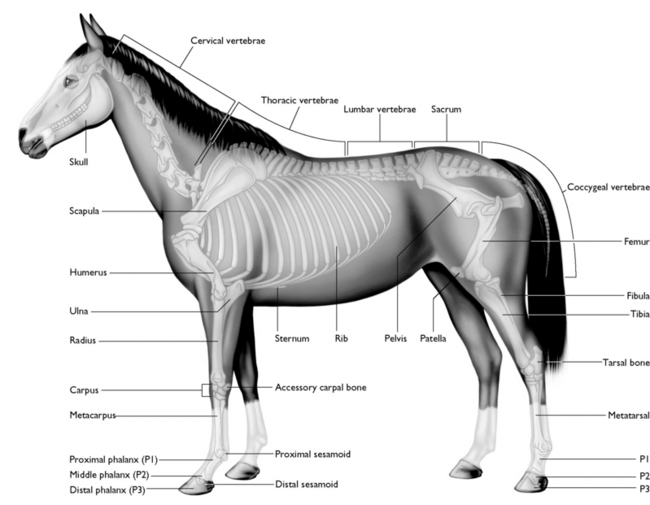
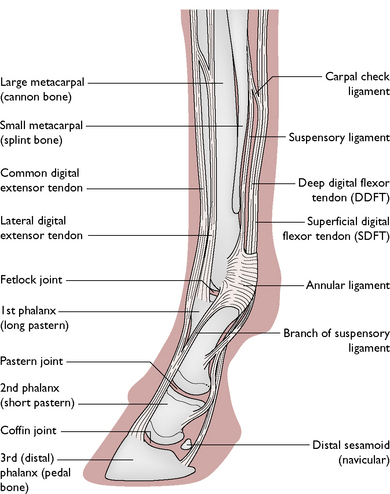
Describe or draw the bones in thoracic and/or hind limb? Feel free to give a general description of how you would do the PE as you go.
BONUS: on what part of the leg do you palpate the radius?
 Bonus: the medial aspect of the Ulna
Bonus: the medial aspect of the Ulna