FLUIDS/ELECTROLYTES
ACID/BASE
MY BEATING HEART
HEART TO HEART
YOU TAKE MY BREATH AWAY
HEART NCLEX
SALTY NCLEX
NCLEX took my BREATH
100
Mr. C was admitted with CHF and labs revealed NA 120
1. why is Mr. C having hyponatremia
2. what are some expected medical / nursing interventions
3. what IV fluid would be anticipated
1. due to fluid overload (dilutional hyponatremia)
2. fluid restriction, furosemide, neuro assessment, seizure precautions, stop IV fluids, cont with NA restriction, daily weight to monitor fluid status
3. hypertonic (3% nacl)
100
what is the normal range for
PH, PCO2, HCO3
which levels are Acidosis, alkalosis
Ph: 7.35-7.45 <acidosis, >alkalosis
Pco2: 35-45 <alkalosis, >acidosis
HCO3: 22-26 <acidosis, >alkalosis
100
Mr. T was diagnosed with
1. what are some priority assessment / why.
2. what are some expected medical / nursing interventions.
3. what symptoms would indicate an emergency
AFIB
1. monitor for CVA s/s--due to risk for clot
2. medical: bb, ccb, AC vs NOAC (Heparin, warfarin, apixaban, rivaroxaban).
nursing: cardiac monitoring, cardiac / neuro assmt, vitals. teaching s/s of CVA & bleeding
3. cardioversion if having hypotension / CP / SOB / MS changes- dizziness, syncope. all indicating decrease cardiac output
100
Mr F. was admitted with right sided fluid heart failure.
1. what are some s/s you expect to assess (SATA)
a. peripheral edema
b. crackle breath sounds
c. pronounced JVD
d. abdominal ascites
A,C,D
peripheral edema, weight gain, fatigue
ascities, enlarged liver,spleen
pronounced JVD
100
The nurse is instructing a hospitalized client with a diagnosis of emphysema about measures that will enhance the effectiveness of breathing during dyspneic periods. Which position would the nurse instruct the client to assume?
Sitting up in bed
Side-lying in bed
Sitting in a recliner chair
sitting up & leaning on an overbed table.
sitting up & leaning on an overbed table. TRIPOD positioning
100

non-modifiable: male, family hx
also DM managment
100
A nurse is assessing a client with hypermagnesemia. Which of the following clinical manifestations should the nurse expect to find?
- A) Increased deep tendon reflexes
- B) Muscle weakness
- C) Hypertension
- D) Hyperactive bowel sounds
B) Muscle weakness - Hypermagnesemia can lead to muscle weakness among other symptoms
along with decrease reflexes, hypotension, constipation. priority is resp depression.
TX: increase fluids / ambulation-forces mag in muscles for function
100
200
Ms C was admitted for hypotension due to dehydration. she was started on 0.9ns at 150cc/hr. the next day, she is complaining of SOB
1. what is possible the cause of her SOB
2. what are some anticipated interventions
3. what are some other symptoms this patient can experience
1. fluid overload from IV fluids
2. stop fluids, elevate HOB, resp assmt (listen to lungs, pulse ox, RR), apply o2 if needed. if needed diuretics, fluid restriction
3. edema, HTN, JVD, Crackles, frothy/reddish secretions, tachycardia, mental status changes, increase weight
200
7.45, 47, 30
7.55, 40, 35
fully compensated metabolic alkalosis by respiratory acidosis
metabolic alkalosis (uncompensated)
200
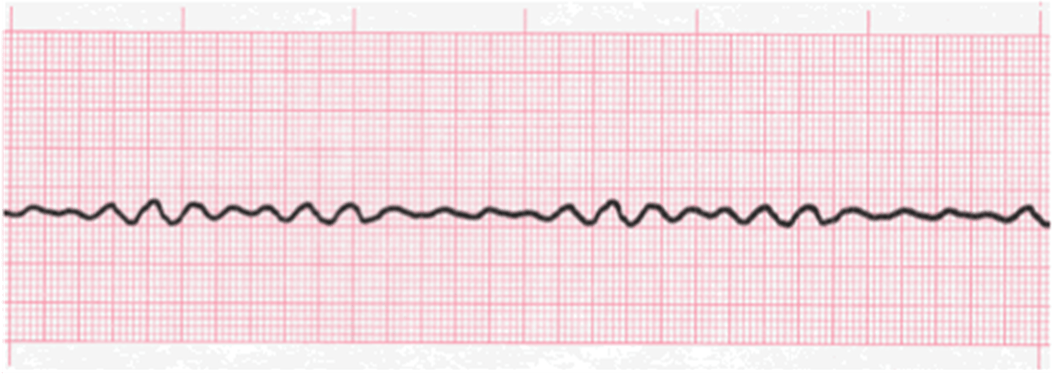
1. what is this rhythm
2. what is the treatment
Vfib
Defibrillation / CPR
200
Ms T was admitted with left sided heart failure. what s/s do you anticipate (SATA)
a. crackles breath sounds
b. liver congestion
c. blood tinge sputum
d. orthopnea
a, c, d.
pulmonary edema, SOB, coughing, confusion, wheezing / crackles, PND, orthopnea, tachycardia
200
Mr M. is admitted with exacerbation of his asthma and is having wheezing.
1. what is your priority assmt
2. what is your priority intervention.
3. what is a preventative measure
1. resp assessment (lungs, pulse ox, rr)
2. albuterol (SABA). issue is bronchoconstriction.
3. avoid triggers
200

200
A client with hypercalcemia is experiencing confusion and lethargy. Which of the following nursing actions is most appropriate? SATA
- A) Encourage the client to increase fluid
- B) Monitor the client’s vital signs closely
- C) Administer a calcium supplement
- D) Provide a high-calcium diet
A) increase fluid to flush out calcium
B) Monitor the client’s vital signs & assessment closely for worsening condition especially arrhythmias, renal calculi
200

1,2,5

confusion, agitation, reslessness = s/s decrease o2 in resp patients.
normal FVC 3000 - 5000ml
300
Mr T. is admitted with + trousseau signs, and complaints of numbness / tingling. he also has been noted to have arrhythmias. labs show electrolyte abnormalities. what electrolyte imbalance do you think he has.
1. hypocalcemia
2. hypercalcemia
3. hyperkalemia
4. hypermagnesium
hypocalcemia
+ numbness / tingling
+ chvosteks / Trouseau sign
give CALCIUM suppplement
300
7.22, 55, 25
7.35, 55, 28
Resp acidosis (uncompensated)
compensated resp acidosis
300
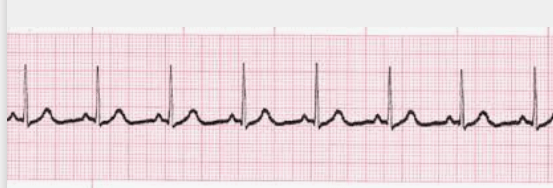
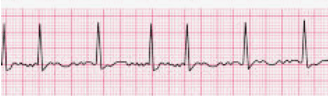
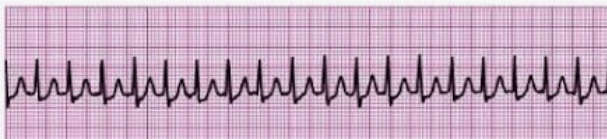
1. what is this rhythm / rate
2. what is the anticipated PR, QRS, QT measurements
SINUS: rate-80. norm 60-100
PR: 0.12-0.20
QRS: 0.08-0.12
QT: < 0.40
300
1. Mr T is admitted with acute CHF and asking what are some interventions that he could do at home to decrease and PREVENT heart failure and decrease hospitalization.
2. what blood levels are checked with heart failure & MI
1. NA & Fluid restriction (decreases hospitalization)
2. BNP (B type natriuretic peptide) with HF. Troponin for myocardial infarction
300
The nurse has a prescription to give a client salmeterol, 2 puffs and beclomethasone dipropionate, 2 puffs, by metered-dose inhaler. The nurse would administer the medication using which procedure?
Beclomethasone first and then the salmeterol
Salmeterol first and then the beclomethasone
Alternating a single puff of each, beginning with the salmeterol
Alternating a single puff of each, beginning with the beclomethasone
Salmeterol first and then the beclomethasone
(LABA / Steroid)
300
decrease perfusion: elevated lft, bun/cr = decrease u/o.
post cath: evaluate 5P's & bleeding
300
A client with hypokalemia is experiencing muscle weakness and shallow respirations. Which of the following nursing interventions is the priority?
- A) Encourage the client to ambulate
- B) place on a cardiac monitor
- C) Administer a potassium supplement
- D) Provide a high-carbohydrate diet
B) place on a cardiac monitor.
will want to provide potassium supplement / foods but priority is ABC
300
also include rest periods, high protein /caloric diet, keep o2 at minimum.
400
1. common side effect with isotonic fluids (0.9ns)
2. common side effects with hypotonic (0.45ns)
3. common side effect with hypertonic (3% Nacl)
1. fluid overload: monitor for pulmonary edema & CHF. give for severe dehydration / hypotension
2. cerebral edema (fluid going into cell): monitor for decrease LOC/mental status changes. give for patients with hypernatremia needing IV fluids
3. fluid overload: monitor for pulmonary edema & CHF. give for severe hyponatremia that is not r/t fluid overload
400
Mr. V was admitted with acute renal failure.
1. what acid base abnormality do you suspect he is at risk
2. what are some symptoms.
3. what electrolyte imbalance is common with this acid-base imbalance
1. metabolic acidosis (due to inability to excrete metabolites, increase hydrogen ions
2. lethargic, confusion, weakness, kussmaul respirations, nauseated, and tingling of the skin, hypotension,
3. hyperkalemia
400
patient is admitted with AMI in the hospital,
1. what are some medications anticipated to be given
2. what diagnostic testing do anticipate will be obtained
3. what would complication would you monitor for post MI
1. MONA
Morphine: pain, decrease anxiety / agitation
Oxygen if needed
ASA: 325mg, chew, thin blood
Nitro: dilate arteries, decrease pain
BB: decrease further ischemia
ACE / ARB: remodeling, low ef
Statin: decrease formation of plaque
2. testing: 12 lead EKG: determine if STEMI, continuous pulse ox, Troponin, Cath
3. Arrhythmia / CHF
400
1. what is expected for treatment of this rhythm
1. Valsalva maneuvers
2. adenosine: IVP fast followed by normal saline push. monitor for aystole for few seconds
3. synchronized cardioversion
400
After the health care provider sees a patient hospitalized with a stroke who developed a fever and adventitious lung sounds, the following orders are written. Which should the nurse implement first?
Anterior/posterior and lateral chest x-rays
Start IV levofloxacin 500 mg every 24 hours now
Complete blood count with differential
Sputum specimen for Gram stain and culture and sensitivity
Sputum specimen for Gram stain and culture and sensitivity
400
DASH: emphasize fruits / veg, whole grains, low fat dairy
also assess for weight control, smoking, exercise, and Medication compliance
400
which patient is at risk for Metabolic Acidosis (SATA)
1. patient with vomiting due to Gastritis
2. type 1 diabetic with blood sugars at 550
3. patient admitted with wbc 30 & positive blood cultures
4. patient admitted with COPD exacerbation
2: DKA
3: Sepsis
400
what is the priority treatment
what are some preventative measures
1,2,5

immune compromised patients sometimes wont have a fever
priority: ABX. check culture first
preventative: hand washing, sunction prn, spirometry (C& DB), ambulate (turn q2)
500
Mrs. L. missed her dialysis for 2 days straight and now is having arrhythmia issues.
1. what electrolyte imbalance do you think she might be experiencing?
2. while waiting for dialysis, what else can we administer. what assessment do we need to perform before administrating
3. what are some nursing interventions
1. hyperkalemia
2. sodium polystyrene sulfonate (monitor bowel),
IV insulin/bicarb/d50/calcium gluconate
3. place on cardiac monitor, frequent electrolyte monitoring
**Furosemide is only if your kidneys are working**
500
Mr R. was admitted with panic attack.
1. what acid base balance is he at risk for
2. what are some s/s to expect
3. would be some anticipated treatment plans
4. what is anticipated electrolyte imbalance
1. resp alkalosis
2. dyspnea, dizziness, numbness/tingling, tremors
3. breathing in bag, benzo, try to do calm patient down
4. hypokalemia
500
patient called your office complaining of mid sternal chest pain with diaphoresis during mowing of grass. he also lets you know that he had chinese food few hours ago.
1. is he having angina vs GERD
2. what would be other associated symptoms
3. what would be your recommendation for treatment since he is home
CHEST PAIN (angina)
-cp/sob, diaphoresis, pain radiating to jaw/back/arm, tachycardia, dyspnea, dizziness, palpitations, fatigue, mild temperature
-STOP ACTIVITY (decrease o2 demand to heart muscle), NTG sl (how to give it), 911 if CP not resolved,
500
What are rhythms that you would do the following interventions
1. synchronized cardioversion
2. defibrillation
3. pacemaker
4. CPR
1. Afib, Aflutter, SVT, Pulse VT
2. Pulseless VT, VF, torsades
3. Bradycardia
4. PEA, Asystole
500
what type of breathing is recommended for patients having COPD / Emphysema
WHY
purse lip breathing.
strengthen lung muscle & extends expiratory phase to eliminate CO2
500
always assess for the 5 P's
1. pain
2. pallor (pale, cold)
3. paresthesia (numbness/tingling)
4. pulselessness (check cap refill)
5. Paralysis (of extremity)
500
A nurse is assessing a client with hypomagnesemia. Which of the following clinical manifestations should the nurse expect to find?
- A) Bradycardia
- B) Muscle cramps and tremors
- C) Decreased deep tendon reflexes
- D) Hypotension
what patient population is at risk for hypomagnesemia
B) Muscle cramps and tremors - Muscle cramps and tremors are common manifestations of hypomagnesemia.
ETOH
500
what assessment data indicate to the nurse the patient needs immediate attention
1. patient s/p thoracentesis with pulse ox 95%
2. patient s/p thoracentesis with complaints of SOB and sats 98%
3. patient s/p thoracentesis with right sided tracheal deviation
4. patient s/p thoracentesis with mild sq emphysema on right side
3. patient with right sided tracheal deviation is emergent since that is a sign of tension pneumothorax.
2 & 4 would also be a concern but patient 3 is the immediate concern at this time.