Primary Survey
Airway & Thoracic Trauma
Shock & Hemorrhage
Head, Spine & Neuro Trauma
Trauma Pearls (Mixed High-Yield Concepts)
100
The components of the PRIMARY survey. (2026 ATLS edition)
x - exsanguination, external hemorrhage
Airway with cervical spine protection,
Breathing
Circulation with hemorrhage control
Disability
Exposure/Environmental control
100
The FIRST priority in EVERY trauma patient?
Establish and maintain a patent airway WHILE protecting the cervical spine.
100
The most common cause of shock in trauma.
Hemorrhage
100
What the "D" in xABCDE stands for.
Disability (Neurologic Assessment)
100
The imaging study routinely performed during the primary survey to evaluate for free fluid.
FAST exam
200
This should be treated IMMEDIATELY if identified in the primary survey.
Any life-threatening problem before moving to the next step.
200
The GCS score that generally indicates the need for definitive airway management?
GCS ≤8
200
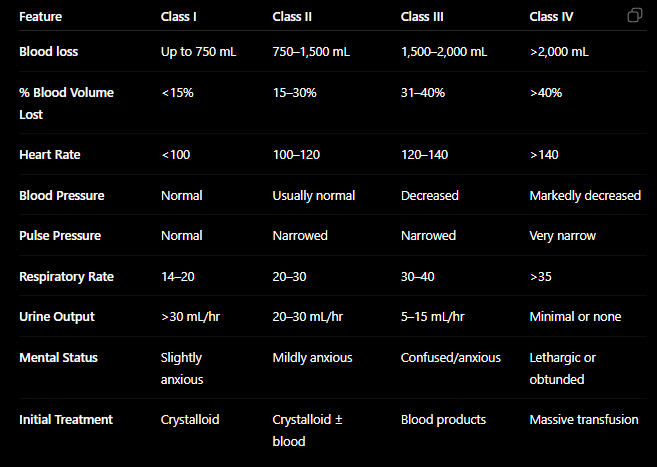
The four classes of hemorrhagic shock.
Classes I-IV
200
The three components of the Glasgow Coma Scale.
Eye Opening
Verbal Response
Motor Response
200
The three components of the lethal triad.
Hypothermia
Acidosis
Coagulopathy
(Now may be changing to "diamond of death": all three plus hypocalcemia)
300
The next step when a trauma patient has absent breath sounds on the left, hypotension, and JVD.
Immediate needle or finger thoracostomy for suspected tension pneumothorax.
300
The preferred initial treatment for an open pneumothorax.
Three-sided occlusive dressing followed by chest tube placement away from the wound.
300
The FOUR major places to look for blood loss in trauma.
Chest
Abdomen
Pelvis
Long bones/soft tissue
300
The first imaging study of choice for suspected traumatic brain injury.
Non-Contrast CT head
300
The blood pressure goals in ages 15y and up for a TBI.
Systolic ≥ 100 mmHg
400
The intervention performed immediately AFTER exposing the trauma patient.
Prevent hypothermia by covering the patient and using warming measures.
400
The amount of blood that defines a "massive hemothorax".
1,500 mL immediately or >200 mL/hour for 2–4 hours after chest tube placement.
400
The blood product type(s) that should be given during massive transfusion.
Balanced blood product resuscitation (approximately 1:1:1 PRBCs:FFP:Platelets)
400
The classic signs of INCREASED intracranial pressure.
Cushing triad:
- Hypertension
- Bradycardia
- Irregular respirations
400
Its the moment SECONDARY survey should begin.
Only after completion of:
1) Primary survey
2) Resuscitation
3) Stabilization
500
The SIX life threatening thoracic injuries identified during primary survey.
- Airway obstruction
- Tension pneumothorax
- Open pneumothorax
- Massive hemothorax
- Flail chest
- Cardiac tamponade
500
Four indications for immediate endotracheal intubation.
Any Four:
- GCS ≤8
- Airway obstruction
- Apnea
- Hypoxia despite oxygen
- Severe facial trauma
- Inability to protect airway
- Respiratory failure
500
The time frame (from time of injury) that TXA should be given to patients with significant bleeding.
3 hours.
BONUS: What is the mechanism of action of TXA? :)
500
What you should expect in a trauma patient that suddenly develops a unilateral fixed dilated pupil and decreasing GCS.
Impending cerebral herniation.
500
List four (of many) indications for transfer to a trauma center.
- Hemodynamic instability
- Severe head injury
- Penetrating torso trauma
- Major burns with trauma
- Multiple long bone fractures
- Pelvic fractures
- Spinal cord injury
- Need for resources unavailable at current facility