Crystals Clear
Uric Acid Trip
Inflammation Nation
Toe-tally Gout
Food & Lifestyle
100
These gout crystals demonstrate strong negative birefringence under compensated polarized light microscopy.
What are monosodium urate crystals?
100
At physiologic pH and temperature, urate exceeds its solubility threshold at approximately this serum concentration.
What is ~6.8 mg/dL? (7)
100
Noninferiority randomized trial tested allopurinol vs febuxostat
what is STOP-GOUT
Flare was a primary endpoint not just SUA
100
Lower temperature and reduced solubility explain why this anatomic characteristic predisposes distal joints to gout.
What is decreased temperature in peripheral joints?
100
Radiologic finding resembleing a fruit found on gout xray
 Apple core appearance
Apple core appearance
200
Blackbox warning for febuxostat
risk of DRESS in some countries
In US; CV risk
- CARES trial Although criticized d/t lots of drug discontinuation an loss-to-f/u
-FREED AND FEATHER RCT: NO CV RISK CONCERN
FAST TRIAL noninferior IN CV RISK
200
When should tx of asymptomatic hyperuricemia be considered
In the absence of symptomatic gout flares or tophi, there are currently no widely accepted indications for the
treatment of asymptomatic hyperuricemia. An exception to this may be in those at high risk for the development of
tumor lysis syndrome (e.g., patients with leukemia initiating chemotherapy).
200
TEst that should be ordered before starting Southeast and east asians/African Americans on Allopurinol
HLA5801; associated w/ starting dose highest risk in first 6 months
Start low; 100mg qd titrate up
50mg qd in CKD pts >4; can titrate to >300mg/d even with renal impairment
Target < 6 sua to avoid therapeutic inertia
200
The classic first MTP joint involvement is referred to by this Latin term.
What is podagra?
200
Gout Flare and CV risk
People with CV event = 2x increase to have gout flare within 60 days prior
Gout flares increase risk of CV risk likely d/t inflammation
300
What percent of pt's at allopurinol 300mg/d fail tx
50% of pts need a dose higher than 300mg/d
300
Can serum urate levels be used to diagnose gout?
Serum urate levels alone cannot be used to diagnose gout. Although serum urate levels are elevated (>6.8 mg/
dL) at some time in almost all gout patients, serum concentrations are normal at the time of an acute flare in up
to one-third (false-negative results). This appears to be in part due to interleukin (IL)-6 generation, which exerts a
uricosuric effect. It is equally important to recognize that many individuals may have hyperuricemia in the absence
of gout (false-positive results).
300
Gout flares can be precipitated with the initiation of ULT. How can this risk be minimized?
Antiinflammatory prophylaxis is recommended to mitigate the risk of gout flares precipitated by initiation of ULT
and should be initiated concomitantly or prior to ULT. Agents most commonly used in prophylaxis include low-dose
NSAIDs (e.g., naproxen 250 mg twice daily) or oral colchicine (0.6 mg once or twice daily). In elderly patients or
those with a GFR of 30 to 50 mL/minute, colchicine doses may need to be reduced (0.6 mg/day or every other
day) and avoided all together with more advanced CKD (particularly as colchicine cannot be removed by dialysis).
Low-dose glucocorticoid treatment (e.g., prednisone 5–10 mg/day) can be used for prophylaxis in those intolerant
to or unable to take NSAIDs or colchicine. Although shown to be efficacious in prophylaxis with ULT initiation, the
role of IL-1 inhibition is uncertain, given the poorly defined risk/benefit ratios.
Prophylaxis should be continued for the first 3-6 months of ULT, as shorter periods have been associated
with rapid increases in flare rates following discontinuation of prophylaxis.
300
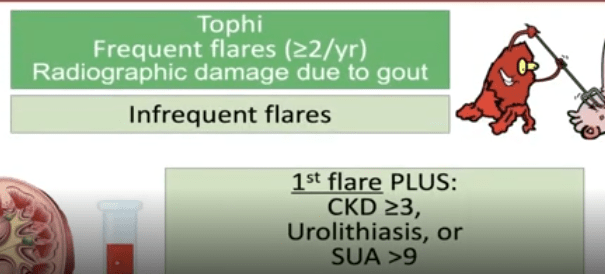
Indications for ULT
300
First step in ULT failure
assess adherence to ULT (and ppx), ensure adequate dose titration
400
What lab should be checked before starting IV pegloticase
Check G6PD prior to initiation
400
Most common nidus for nephrolithiasis
What is Urate
- A Nidus for Calcium Stones (Epitaxy): Urate crystals act as a surface (nidus) on which calcium oxalate and calcium phosphate can precipitate. This process, called epitaxy, means that even in mixed stones, the initial core is often a urate crystal.
400
This inflammasome is activated by urate crystals and drives IL-1β–mediated inflammation in gout.
What is the NLRP3 inflammasome?
400
What medication can be added to prevent antibody formation against IV pegloticase
Methotrexate
400
Modification of lifestyle factors for gout (4)
Weight loss; alcohol; purines (meat); HFCS
*High heat low humidity can cause more evaporative loss and can trigger gout
Omega 3's associated with reduced flares, Cherries/ cherry extracts also observed for lower flares
500
Who was Podagra
In mythology, Podagra was the foot-torturess born of the seduction of Venus by Bacchus. This terrible-tempered
virgin goddess even inspired fear in Jove!
500
Colchicine in renal dz w/ statins can cause
What is neuromyotoxicity
500
MGMT of flare in CHF pt and why?
Il-1 antagonist canakinumab
Dexamethasone d/t lowest mineralcorticoid effect
500
Classes of medications contraindicated in CKD pts on colchicine that can be fatal
P-glycioprotein or CY3A4 inhibitors
eg clarithromycin, certain antifungals, certain CCBs (verapamil, diltiazem), GRAPEFRUIT JUICE
AVoid using for flare mgmt if Already on it for ppx in pts with renal insufficiency
500
Hyperinsulinemia worsens hyperuricemia primarily by increasing this renal process.
What is proximal tubular urate reabsorption?
SGLT2i have been demonstrated to lower urate, but no trial data, seems to reduce incident and recurrent gout