Wound Care Guidelines
Who you gonna consult?
Take a picture it
lasts longer!
lasts longer!
Odds and Ends
Back to Basics
100
Wound care guideline for treatment after placing a wound care consult.

What is skin prep daily and PRN, open to air.
100
Patient with severe diabetic ulcers.
What is podiatry service.
100
Day of the week that staff update pressure injury pictures in the media.
What is Wednesday.
100
4 eyes in 4 hours.
What is 2 RN skin check completed and documented on admission to any unit, transfer to any unit, and after a procedure.
100
A Braden scale indicating high risk.
What is 18 or less.
200
Your patient is admitted with this and states they have had it for 2+ years. Upon assessment there is scant purulent drainage, and the wound bed is pale with a callous. Using the wound care guidelines you recommendation would include these items.
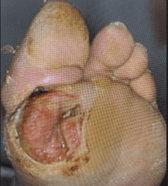
What is a podiatry consult and for the interim, lightly pack with Vashe or Dakins solution moistened kerlix; change twice daily.
200
Venous stasis ulcers that are deteriorating since admission 6 days ago despite following the wound care guidelines.
Wound care and consider vascular consult.
200
An item that should be present in the media photo when uploading to the chart.
What is a ruler with the patient's name and birthdate on it.
200
Risk notification of wounds on admission, transfer, new wound or if a wound deteriorates
What is Safety Net.
200
All heels should be this.
What is offloaded.
300
Recommendations using wound care guidelines for no drainage and dry wound bed.

What non-adherent petrolatum gauze or Medihoney.
300
Patient has a rash that covers their chest, arms and back.
What is notify the covering provider and possible Dermatology Consult
300
Criteria for Wound Care consult.
What is Stage 3/stage 4 PI, unstageable PI, evolving DTIs on sacrum, stable diabetic foot wounds, new ostomy patients, complex fistulas, full thickness wounds and xylazine wounds with large areas of necrosis/malodorous.
300
An important assessment strategy when assessing a vulnerable area at risk.
What is good lighting.
300
This area is nonblanchable.

Stage 1 pressure injury.
400
Describe the wound edges.
What is macerated and epibole (rolled).
400
Patient has an extensive wound over their sacrum.
What is Wound care.
400
Important aspects of a wound assessment.
What is palpation, signs of infection (erythema, induration, crepitus), pain associated with wound area.
400
Hospital acquired injuries are considered these two things.
What is a never event and a nursing sensitive indicator.
400
Sacral and gluteal cleft with diffuse blanchable erythema and partial thickness tissue breakdown.
What is moisture damage.
500
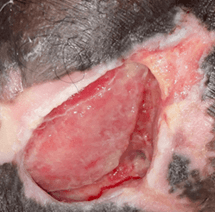
Goal of wound care and consult recommendation for a wound base that is gray and black with surrounding erythema.

What is debridement of dead tissue.
Options include topical treatment for debridement and/or surgical consult for debridement.
500
Newly dehisced surgical wound.
Contact covering provider, surgical service if applicable.
500
Chart flow when finding or assessing a wound.
What is a properly identified photo, an LDA created/updated, orders for treatment using the guidelines, and possibly a wound care consult placed.
500
Head to toe assessment should focus on these areas.
What is bony prominences ie occiput, elbows, sacrum/coccyx, heels, etc.
500
Oncoming report to next shift description for this wound.

Stage 4 pressure injury. Report wound characteristics such as tissue color, odor, and the presence of necrosis.