Pulmonology
Gastroenterology
General IM
Critical Care
Take a good look
100
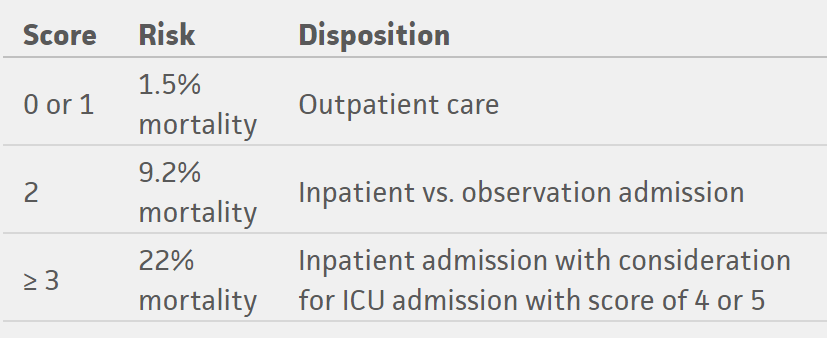
Specific quantitative criterion represented by R in the CURB-65 score
RR > 30/min
C= confusion
U= uremia i.e. BUN >19
R as above
B = BP i.e. hypotension <90/60
100
To reduce false-negative urea breath test results, the patient should be off antibiotics for this amount of time before eradication testing for H. pylori is done
4 weeks
100
USPSTF recommends this cervical cancer screening interval when cotesting cytology and HPV testing
every 5 years
May start at age 30
If solely cytology, repeat q3 years
100
Most antecendent of critical illness polyneuropathy
Sepsis
100
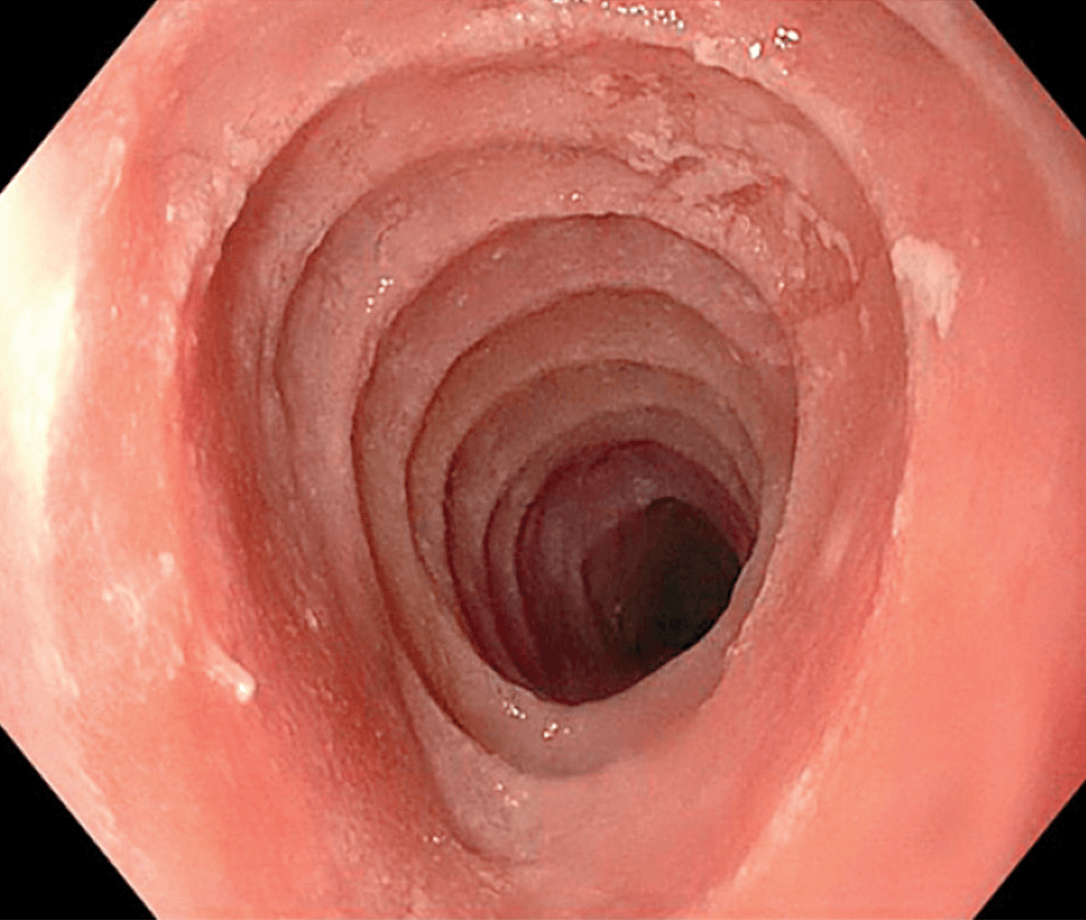
Treatment?
Budesonide or Fluticasone (swallowed and aerosolized)
200
Liver condition that may result in a brown effusion
Amebic abscess
200
Most common myelodysplastic syndrome associated Budd-Chiari syndrome
Polycythemia vera
200
CDC recommends one-time screening for Hep C for persons born during this interval
1945-1965
200
Initial preferred ventilation strategy for cardiogenic pulmonary edema
NIPPV
200

What is the likely diagnsois?
Psoriasis
Other nail changes:
yellow/pink discoloration
Nail plate crumbling
Splinter hemorrhages
300
Timing of initial imaging to follow up for 4mm solid pulmonary nodule on CT scan in high risk patient
12 months
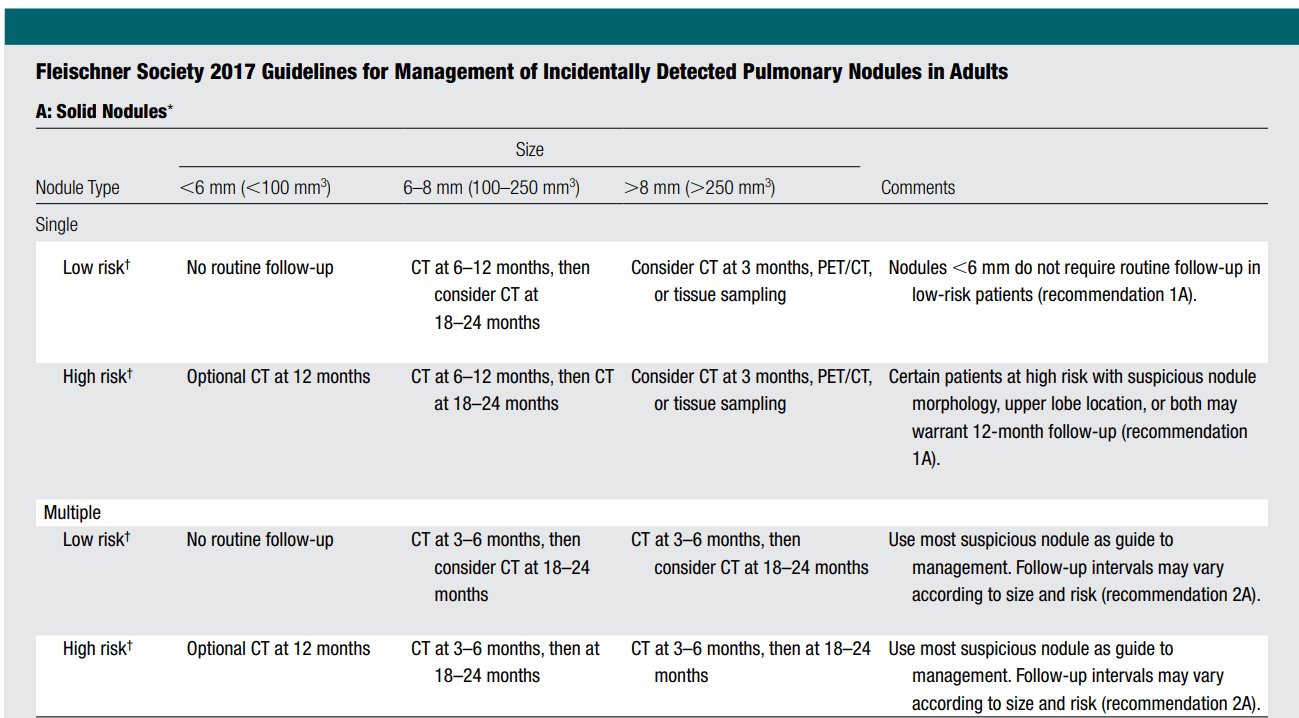
High risk factors: include older age, heavy smoking, larger nodule size, irregular or spiculated margins, and upper lobe location.
300
Condition associated with periodic acid-Schiff-positive macrophages and negative acid-fast stain
Whipple disease
Recall sx:
- diarrhea
- weight loss caused by malabsorption
- Arthralgias
- fatty or bloody stools
- abdominal cramps or bloating felt between the chest and groin
- loss of appetite
- fever
- fatigue, or feeling tired
- weakness
People with a more advanced stage of Whipple disease may have neurologic symptoms—
- vision problems.
- memory problems or personality changes.
- facial numbness.
- headaches.
- muscle weakness or twitching.
- difficulty walking.
300
BONUS QUESTION
Guess that tune - Title and Artist
All the stars
Kendrick Lamar & SZA
300
PO2/FIO2 Berlin Criteria for severe ARDS
< 100
300

44 year old woman w/ acute chest pain w/ several months of progressive dyspnea.
O2 sat is 92%, diminished breath sounds on right
Likely diagnosis?
Lymphangioleiomyomatosis
Typically affects women in 30s-40s
Activation of mTOR w/ formation of numerous thin-walled cysts lined with spindle cells co-expressing smooth muscle and melanocytic markers.
400
Diagnosis in ventilated patient for hypotension, decreased left breath sounds and left deviated trachea
Right main bronchus intubation
400
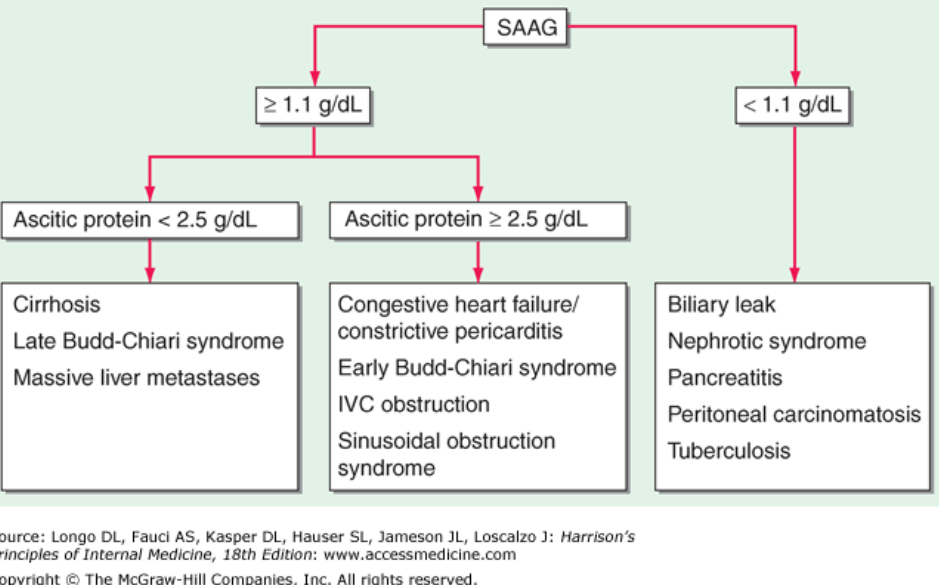
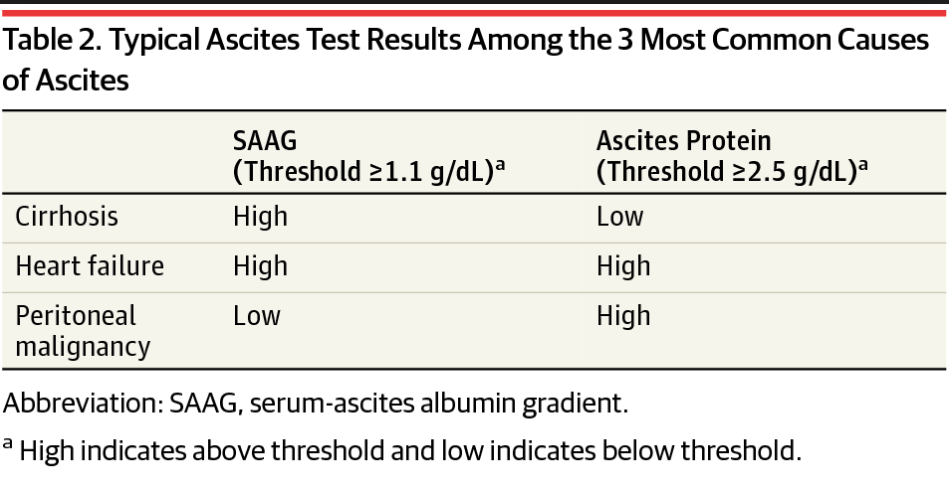
SAAG and ascitic protein concentration thresholds associated with constrictive pericarditis
SAAG > 1.1
Ascitic Protein > 2.5 g/dl
400
Ipsilateral abscence of this reflex is 99% sensitive for testicular torsion
Cremasteric reflex
400
Acid-base disorder characteristic of propofol infusion syndrome
Metabolic acidosis (high AG)
400

21 y/o female w/ HIV and prior IVDA CD4 count of 400, not on ART.
1 week hx of fever, chest pain and hemoptysis.
What are these findings?
Pulmonary abscesses
BC grew MSSA
ECHO showed fluttering vegetation on the tricuspid valve
500
TB test for lymphocytic pleural fluid when initial smear and culture TB are negative
Adenosine Deaminase
sensitivity 97.05%
specificity 95.83%
500
Most consistently effective biological therapy for recurrent and antibiotic refractory C. diff
Fecal microbiota transplantation
500
 Name of this painful drug eruption
Name of this painful drug eruption
Fixed drug eruption
Painful purple patch occurs in the same location repeatedly - usually the lips, genitals and hands
Common rx culprits:
NSAIDs
Pseudoephedrine
Sulfa drugs
500
79 year old gentleman on SBT. Hx of COPD. Admitted 3 days prior for fever, shortness of breath,wheezing and productive cough. Failed NIPPV and was intubated.
MRSA pneumonia diagnosis.
On SBT, two hours later PEEP of 5 and FiO2 of 40%, afebrile, 153/76 BP, HR 98/min, RR of 18. Tidal volume averaging 300cc.
Following commands and lifts head off bed. Left-sided crackles and normal S1 and S2.
CXR w/ unchanged left base infiltrate.
Extubate or not and if so to what?
Extubate to NIPPV
500
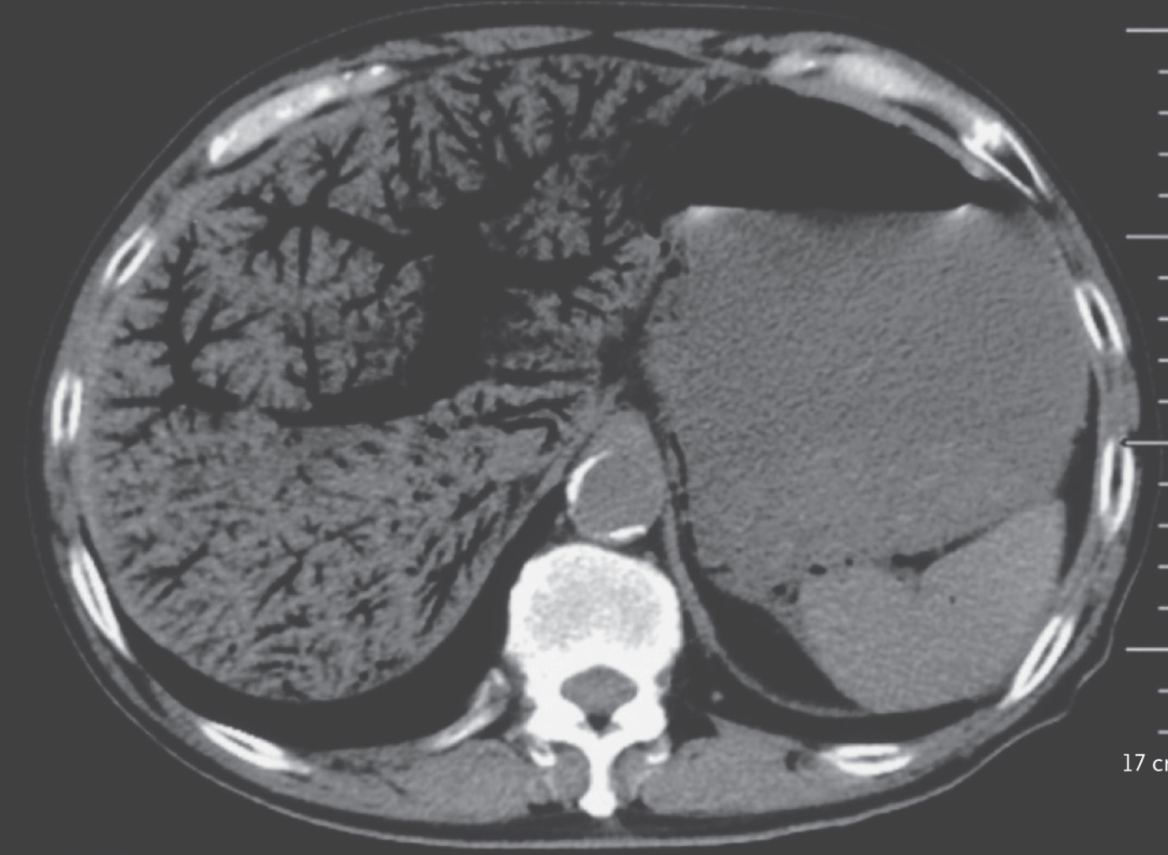
A 72 year old man, 11 hour hx of periumbilical abdominal pain, inability to pass flatus.
VS: HR 155, BPD 83/52. Abdomen diffusely tender w/ most severe pain in the RUQ.
WBC 22k, pH of 7.27, Lactic acid of 8.
CT findings as above.
Most common underlying cause?
Bowel ischemia
Portal venous gas most commonly associated w/ this. poor prognostic sign
Other conditions:
IBD
Infections