Neurons & Associates
Heart Hustler
Lung Whisperer
Kidney Keeper
Bloody Wine
Gut Guru
Endo DJ
Legs are speaking
100
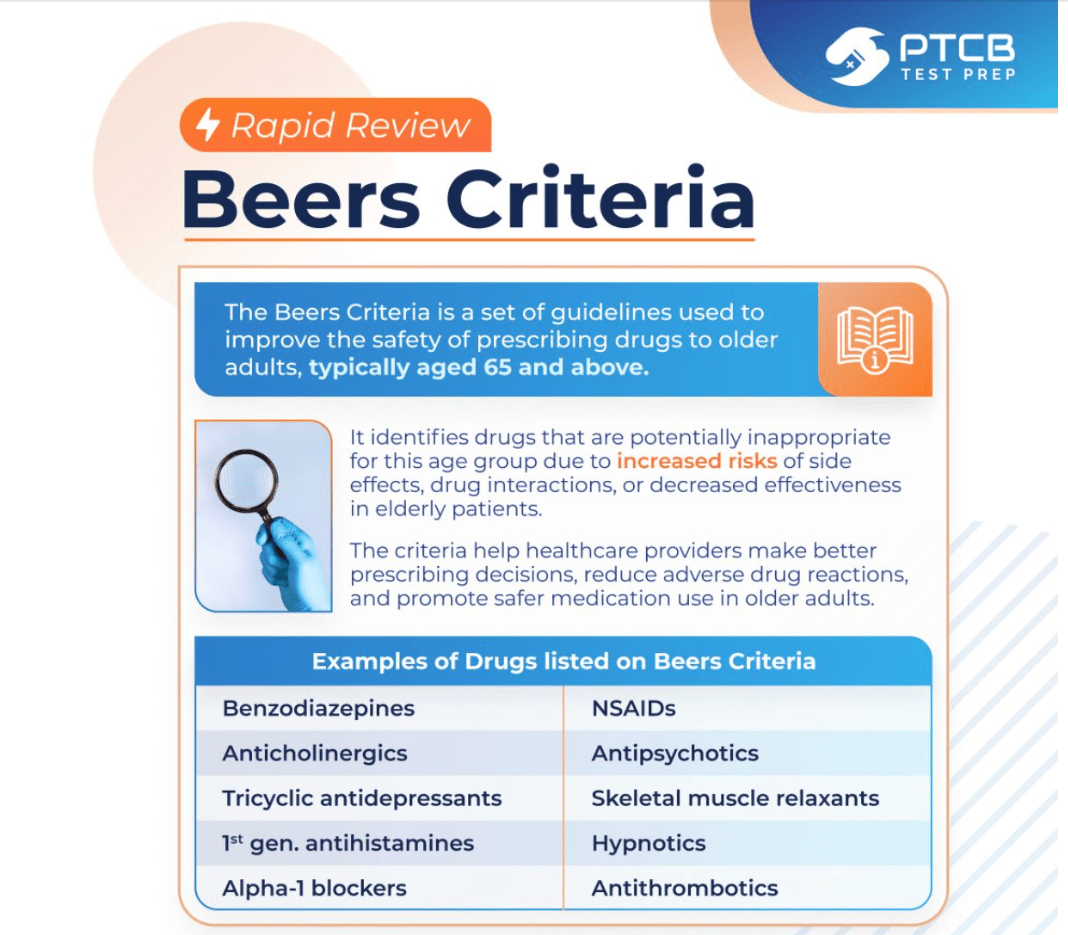
What criteria is used to identify potentially inappropriate medications for adults 65 and older?
100
Classic parameters of severe aortic stenosis?
Aortic valve area: ≤ 1.0 cm2
Transaortic velocity: ≥ 4.0 m/second
Mean aortic pressure gradient: ≥ 40 mm Hg
Last two are variable, depending on subdivision
100
In acute COPD exacerbation, characterized by worsening dyspnea and cough and an increase in sputum volume and purulence, without systemic symptoms. While the results of sputum culture are pending, empiric treatment?
Oral antibiotic such as a fluoroquinolone
Has complete or partial coverage for typical pathogens
100
What is the minimum increase in serum creatinine within 48 hours required to diagnose AKI?
≥ 0.3 mg/dL
A small but acute rise in creatinine is enough to diagnose AKI if it occurs rapidly (≤48h).
100
How to diagnose Neutropenic fever?
Neutropenic fever is defined as a temperature ≥ 38°C (100.4°F) for ≥ 1 hour
or
≥ 38.3°C (101°F), combined with an Absolute Neutrophil Count (ANC) < 500/mm3

100
Diagnostic criteria for Severe C. diff?
leukocytosis ≥ 15,000/mm³
or
serum creatinine ≥ 1.5 mg/dL
100
42 yo woman presents with HTN, muscle weakness, and fatigue. Labs show hypokalemia, metabolic alkalosis and low plasma renin.
What is the next best step to confirm the diagnosis?
Measure the aldosterone-to-renin ratio (ARR)
The ARR is the initial screening test for primary hyperaldosteronism.
- High aldosterone + low renin → elevated ARR → suggests Conn syndrome
- Followed by confirmatory testing (e.g., saline suppression test)
100
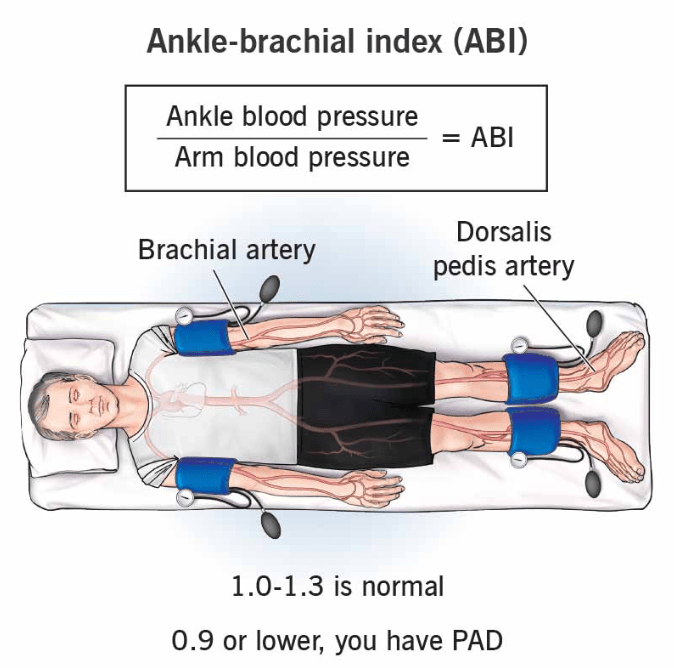
What ABI value is diagnostic for PAD?
An ABI ≤ 0.90 is diagnostic for peripheral artery disease
200
What test is used by patients at home to monitor the progression of macular degeneration?
Amsler grid
200
Which electrolyte abnormality is associated with poor prognosis and higher mortality in patients with D-CHF?
Hyponatremia
In D-CHF, reduced cardiac output triggers increased ADH secretion, causing excess free water retention. This dilutes serum sodium and leads to hyponatremia, which is associated with worse heart failure severity, poor prognosis, and higher mortality.
200
Mention 3 minor criteria for Severe Community-Acquired PNA?

200
What urine output threshold defines AKI according to KDIGO?
<0.5 mL/kg/hr for ≥6 hours
Oliguria is a key early marker of AKI and part of diagnostic criteria.
200
What lab finding differentiates iron deficiency anemia from anemia of chronic disease?
Low ferritin (iron deficiency)
VS
normal/high ferritin (ACD)
Key: Ferritin reflects iron stores
200
A hospitalized patient on long-term PPI for stress ulcer prophylaxis develops chronic diarrhea, bloating, and malabsorption. Labs show ↑ folate and ↓ vitamin B12. Most likely Dx?
PPIs → ↓ gastric acid → loss of antibacterial barrier → small intestinal bacterial overgrowth (SIBO)
Bacteria produce folate (↑), and consume B12 (↓) → classic exam pattern
200
What endocrine pathology should be suspected in a patient who underwent PCI a few days ago, and now develops anxiety symptoms with sinus tachycardia on ECG?
Thyrotoxycosis
Patients exposed to a clinically significant amount of iodine-containing contrast medium are at risk for contrast-induced thyrotoxicosis if they have underlying thyroid disease (MC Multinodular goiter)
200
Four days after a craniotomy, patient developed severe pain and swelling in his right leg, and DVT is diagnosed. What is the most appropriate treatment?
IVC filter
IVC filters are indicated in:
high risk of thromboembolism who have absolute contraindications to anticoagulation
or complications from anticoagulation
as well as those who have not responded to anticoagulation
300
In patients with non-disabling acute ischemic stroke, for how many days is DAPT recommended?
Short-term DAPT (21 days) reduces early recurrent stroke risk while minimizing bleeding
Prolonged use increases hemorrhagic risk without added benefit.
Transition to SAPT after 21 days
300
What medication should be avoided in a suspected variant (Prinzmetal) angina?
Beta-blockers are generally contraindicated in variant (Prinzmetal) angina because they can cause unopposed adrenergic stimulation, which worsens coronary artery vasospasm.
Variant angina is caused by spasm, not plaque, and beta-blockers block mediated vasodilation, leaving mediated vasoconstriction unopposed, thus worsening the spasms.
300
In acute asthma exacerbation, what is the indication for IV magnesium sulfate?
Poor response to SABA + FEV1 <60%
IV magnesium is used in moderate–severe exacerbations when there is inadequate response to bronchodilators, helping with smooth muscle relaxation
300
A patient with small cell lung cancer develops SIADH. How is the behavior of serum sodium and urine osmolality with this condition?
Low serum sodium with high urine osmolality
SIADH causes euvolemic hyponatremia due to excess ADH → water retention → diluted serum (low Na) but concentrated urine (high osm)
kidneys to reabsorb free water, leading to concentrated urine
300
What is the molecular target of imatinib in chronic myelogenous leukemia (CML)?
BCR-ABL tyrosine kinase
Key: t(9;22) Philadelphia chromosome → constitutive kinase activation.
300
A young male with ulcerative colitis presents with cholestatic liver enzymes. MRCP shows multifocal strictures with a “beaded” appearance of the bile ducts. What is the most feared malignancy associated with this condition?
Cholangiocarcinoma
Primary sclerosing cholangitis (PSC) is strongly associated with ulcerative colitis and leads to progressive fibrosis of intra- and extrahepatic bile ducts.
Major complications include:
- Cholangiocarcinoma (high risk)
- Cirrhosis → liver failure
300
As per new PREVENT-ASCVD risk, what is the target for LDL-C in very high risk patient
For individuals with ASCVD who are at very high risk of ASCVD events, the LDL-C goal should be less than 55 mg/dL or ≥50% reduction from untreated baseline for secondary prevention of cardiac events.
https://newsroom.heart.org/news/accaha-issue-updated-guideline-for-managing-lipids-cholesterol
300
Which antithrombotic regimen, known as the COMPASS regimen, is recommended for symptomatic PAD to reduce major adverse cardiovascular and limb events?
Low-dose rivaroxaban 2.5 mg BID plus aspirin 81 mg daily
It was more effective than aspirin alone in reducing major cardiovascular events in stable CAD/PAD, but with a higher risk of major bleeding
400
Before starting natalizumab in a patient with multiple sclerosis, which infection risk marker should be screened for?
JC virus (anti-JCV antibodies)
Natalizumab increases the risk of progressive multifocal leukoencephalopathy (PML), a serious opportunistic brain infection caused by JC virus reactivation
400
Two Contraindications for MRAs
1. eGFR < 30 mL/min/1.73m2
2. Serum K+ > 5.0 mEq/L
400
According to GOLD 2026, what is the recommended initial therapy for COPD patients, and when should triple therapy be started upfront?
Dual bronchodilator (LABA + LAMA); start triple therapy if eosinophils ≥300/µL
GOLD 2026 emphasizes early dual bronchodilation, with escalation to triple therapy in eosinophilic phenotype, reflecting inflammation-driven disease.
Remember: IgE, FeNO, EOS
400
In a patient with severe metabolic acidosis, what arterial pH threshold is considered an absolute indication for emergent hemodialysis despite maximal medical therapy?
pH < 7.20, indicates life-threatening acidemia.
If it persists despite medical management (including bicarbonate), urgent dialysis is required to correct acid-base imbalance.
400
What is the key clinical clue that suggests heparin-induced thrombocytopenia (HIT) rather than other causes of thrombocytopenia?
Thrombosis despite thrombocytopenia
Key: “Clotting, not bleeding” → paradoxical hypercoagulable state.
- Widespread clot formation (arterial + venous)
- Platelet consumption → thrombocytopenia
400
A patient with suspected celiac disease has positive anti–tTG IgA but has already started a gluten-free diet, and symptoms have improved. What is the next best step to confirm the diagnosis?
Gluten challenge followed by duodenal biopsy
Starting a gluten-free diet can normalize serologies and mucosal findings, leading to false-negative biopsy.
To confirm diagnosis → reintroduce gluten (gluten challenge) → then perform duodenal biopsy.
400
A patient on an SGLT2 inhibitor presents with nausea, abdominal pain, and metabolic acidosis, but glucose is <250 mg/dL. What is the diagnosis?
Euglycemic DKA
Key: occurs commonly with SGLT2 inhibitors → promotes glucosuria, so glucose is not markedly elevated.
Diagnosis relies on anion gap metabolic acidosis + ketosis, despite “normal” glucose.
400
In patients with both PAD and diabetes mellitus, which glucose-lowering medication classes are preferred because they provide proven cardiovascular benefit and reduce major adverse cardiovascular events?
GLP-1 receptor agonists or SGLT2 inhibitors
500
A patient with acute ischemic stroke due to large vessel occlusion (LVO) presents within 4.5 hours and is a candidate for mechanical thrombectomy. According to recent evidence, what pre-thrombectomy intervention improves functional outcomes?
IV tenecteplase before thrombectomy
The BRIDGE-TNK trial showed higher functional independence with tenecteplase + thrombectomy vs thrombectomy alone, at the cost of a modest increase in symptomatic ICH
Alteplace and TNK are both Class I now
Selection criteria is now imaging-based
500
In patients with HFrEF, what are the laboratory criteria that indicate initiation of IV iron therapy?
Ferritin <100 ng/mL
OR
ferritin 100–299 ng/mL with TSAT <20%
Iron deficiency in HFrEF is defined by low ferritin or low transferrin saturation, and IV iron improves symptoms, functional status, quality of life, and reduces heart failure hospitalizations; independent of hemoglobin levels
AFFIRM-AHF (ferric carboxymaltose)
500
What is the treatment of choice for Group 4 pulmonary hypertension?
Pulmonary endarterectomy
if the patient is operable. If the disease is inoperable or persistent after surgery, treatment includes riociguat and/or balloon pulmonary angioplasty, and patients generally require lifelong anticoagulation
500
Describe the associated pathology with this microscopic finding?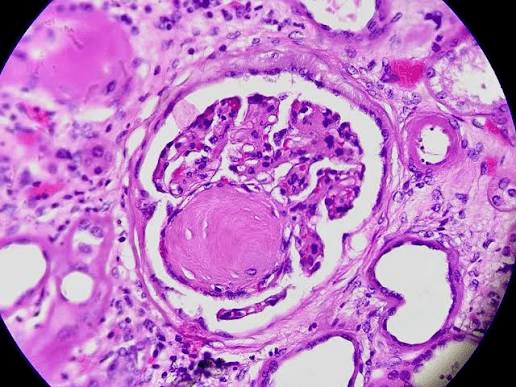
Diabetic nephropathy
Kimmelstiel-Wilson (KW) nodules, or nodular glomerulosclerosis, are hallmark pathological lesions of advanced diabetic nephropathy, characterized by round, eosinophilic, acellular mesangial matrix deposits in the periphery of glomeruli
500
What is the first-line treatment for hyperleukocytosis with symptomatic leukostasis in acute leukemia?
Leukapheresis
Medical emergency—reduces WBC burden rapidly (hydroxyurea also used, but leukapheresis is key in symptomatic cases)
500
In which patients is resmetirom indicated for treatment of MASH?
F2–F3 fibrosis with LSM 8–20 kPa and no cirrhosis
Resmetirom is NOT used in cirrhosis (F4 or LSM >20 kPa). This is a new guideline favorite question.
500
A young patient presents with recurrent pancreatitis, eruptive xanthomas, and lipemic serum. Labs show markedly elevated triglycerides (>1000 mg/dL). What is the underlying defect in familial hyperchylomicronemia?
Lipoprotein lipase (LPL) deficiency (or ApoC-II deficiency)
Familial hyperchylomicronemia = impaired clearance of chylomicrons due to defective LPL or ApoC-II, leading to severe hypertriglyceridemia → pancreatitis risk.
Olezarsen: significantly lowers triglycerides by inhibiting Apolipoprotein C-III (ApoC-III) production in the liver
500
A patient with suspected DVT has a Wells score of 3 and a negative D-dimer. What is the next step in management?
Perform venous ultrasound (US)
In Wells ≥3 (DVT likely) patients, a negative D-dimer does NOT rule out DVT — imaging is required
A (-) US is still concerning for DVT in this pt.