Over-reacting
Stop the Bleed
U so Malignant
Sickle Saga
Baby Now We Got
Bad Blood
Bad Blood
100
This is the standard, weight-based or standard adult intramuscular dose of epinephrine recommended for anaphylactic shock.
0.3 to 0.5 mg (or 0.01 mg/kg)
100
In a hemophilia A patient presenting with a life-threatening intracranial hemorrhage, you need to calculate this factor dose to achieve this target percentage of normal factor activity.
Factor VIII and 100%
100
In Tumor Lysis Syndrome, the massive release of intracellular contents leads to this specific tetrad of metabolic derangements.
Hyperkalemia, Hyperphosphatemia, Hyperuricemia, and Hypocalcemia
Rasburicase/Allopurinol, Calcium Gluconate, K lowering meds.
100
In an adult patient with sickle cell anemia presenting with severe bone pain and a sudden drop in hemoglobin, this specific virus is the most common cause of an aplastic crisis.
Parvovirus B19
Low Reticulocyte Count
100
During a massive transfusion protocol for a trauma patient, the rapid infusion of older, stored packed red blood cells can precipitate this specific, life-threatening electrolyte derangement on the monitor.
Hyperkalemia
As packed RBCs sit in storage, the cells slowly lyse and leak potassium into the surrounding solution. When you rapidly pressure-infuse multiple older units into a crashing patient, you can cause acute, emergent hyperkalemia
200
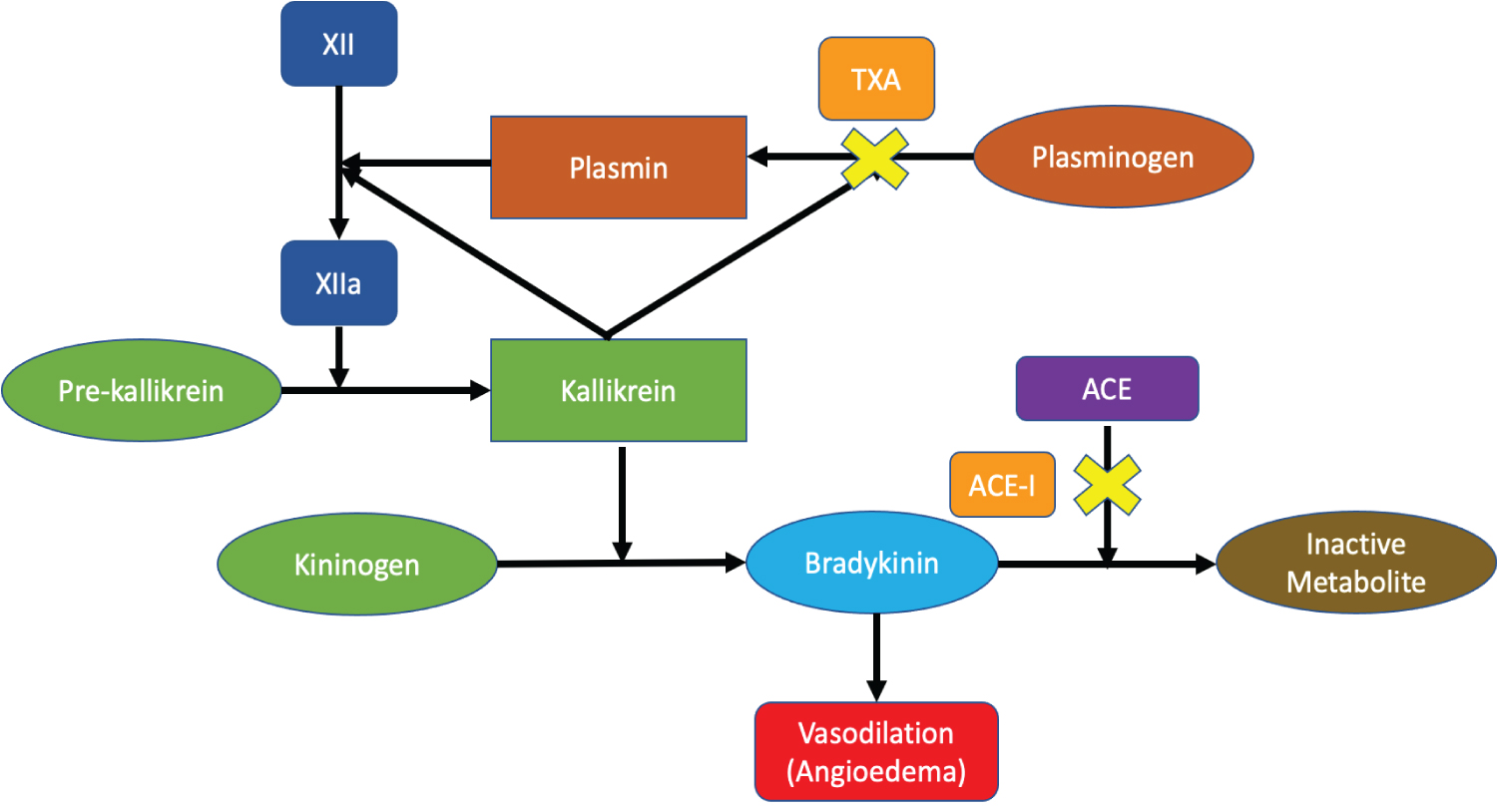
This specific component of the complement system is deficient or dysfunctional in Hereditary Angioedema.
What is C1 esterase inhibitor
200
In a patient with von Willebrand disease experiencing mild to moderate mucosal bleeding, this synthetic hormone is the first-line ED treatment to stimulate the release of stored vWF.
It is also the preferred first line medication for acute life threatening bleeding in a patient on anti-platelet medication.
DDAVP (desmopressin)
0.4 mcg/kg dose
200
This absolute neutrophil count (ANC) threshold officially defines severe neutropenia, making a fever an emergent oncologic threat.
What is less than 500 cells/microL (or <1000 with a predicted decline to <500)?
200
For a pediatric patient with sickle cell disease presenting with fever, this encapsulated organism is the most common and feared cause of rapid, fatal sepsis due to autosplenectomy.
Strep pneumonia
Others include: Salmonella (particularly in older children/bone infections), Haemophilus influenzae type b (Hib), and Staphylococcus aureus.
200
The primary cause of this transfusion related complication is the transfusion of incompatible blood, most frequently due to clerical errors (misidentification of the patient or donor sample), resulting in ABO incompatibility (e.g., A-type blood given to an O-type recipient).
Acute Hemolytic Transfusion Reaction
- Pathophysiology: Donor red blood cells (RBCs) are destroyed by recipient antibodies, leading to intravascular hemolysis, complement fixation, and the release of cellular debris.
- Diagnosis: Confirmed by a positive direct antiglobulin (Coombs') test, evidence of hemolysis (increased plasma/urine hemoglobin), and often, a peripheral blood smear showing RBC destruction.
- Prognosis & Management: Immediate cessation of the transfusion is necessary, followed by aggressive supportive care to manage shock and renal failure. While serious and potentially fatal, prompt intervention can improve outcomes.
300
This synthetic, subcutaneous medication used to treat acute attacks of hereditary angioedema (HAE)
Icatibant
It is a peptidomimetic consisting of ten amino acids, which is a selective and specific antagonist of bradykinin B2 receptors.
300
Both severe liver disease and DIC feature elevated PT/PTT and low platelets, but this specific laboratory marker is characteristically elevated in DIC and normal in liver disease.
D-dimer (or Fibrin Degradation Products)
DIC: consumptive coagulopathy that can cause both micro-thrombotic and hemorrhagic complications.
300
Management of this acute oncologic emergency includes a tyrosine kinase inhibitor (-nibs), hydroxyurea, allopurinol, and leukapheresis (in addition to chemotherapy).
Acute Blast Crisis, > 20% blasts
CML is MOST COMMON
Allopurinol acts to prevent TLS, reduces risk of hyperuricemia.
300
This this penile injectable medication is considered first line therapy for ischemic priapsm, along with corporal aspiration and irrigation.
Phenylephrine
Phenylephrine should be diluted in normal saline to produce a concentration of 100–500 μg/ml. Then, injections of 1 ml aliquots should be performed intracavernosally every 3–5 min for up to 1 h or up to a dose escalation of 1000 μg of diluted phenylephrine
300
This transfusion reaction presents with isolated fever and chills within 1-6 hours of a transfusion and is mediated by recipient antibodies reacting against donor leukocytes.
Febrile Non-hemolytic Transfusion Reaction
Immediate Action and Treatment
- Stop the transfusion: Immediately stop the blood transfusion and keep the line open with saline.
- Notify Blood Bank: Initiate a reaction workup to rule out acute hemolytic reactions.
- Antipyretics: Administer oral acetaminophen (325–500 mg) for fever and discomfort.
Prevention and Future Precautions
- Leukoreduction: Use leukocyte-reduced blood components for future transfusions to reduce the presence of white blood cells that cause the reaction.
- Premedication: While not always necessary, premedication with antipyretics is sometimes used for patients with a history of recurrent FNHTR.
400
This type of Hypersensitivity Reaction is characterized by immune-complex deposition and is associated with diseases such as SLE, Rheumatoid Arthritis, and Post-Streptococcal GN.
Type III
400
This agent is the preferred first line therapy for acute intracranial bleed associated with IV lysis for ischemic CVA (tPA or TNKase).
Cryoprecipitate 10 U IV
Lytic State: In cases of hyperfibrinolysis, Cryo provides fibrinogen to support clot formation
Goal fibrinogen level: maintain fibrinogen levels >150–200 mg/dL
400
First line monotherapy of febrile neutropenia includes this class of IV antibiotic.
Anti-pseudomonal B-lactam.
400
This is the targeted exchange transfusion goal for the percentage of Hemoglobin S in a patient presenting with an acute ischemic stroke or severe acute chest syndrome.
< 30%
400
This potentially fatal reaction occurs when viable donor T-lymphocytes attack an immunocompromised recipient's tissues; it is prevented by irradiating blood products before administration.
Transfusion-Associated Graft-vs-Host Disease (TA-GVHD)
500
This medication, discovered and initially utilized in patients with post partum hemorrhage, can be used in cases of ACE-induced angioedema to reduce bradykinin levels.
TXA
500
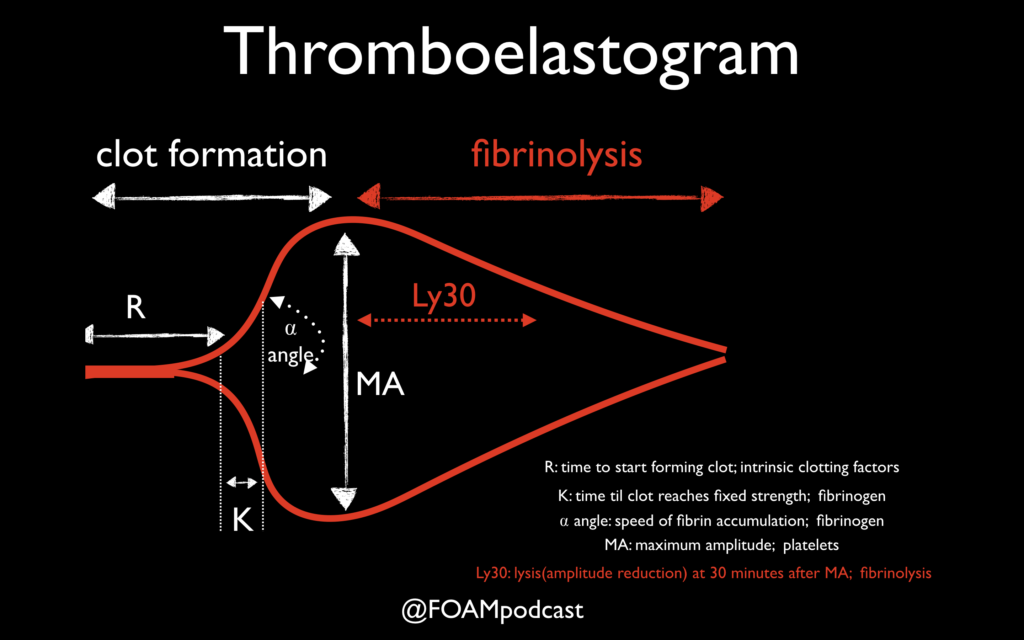
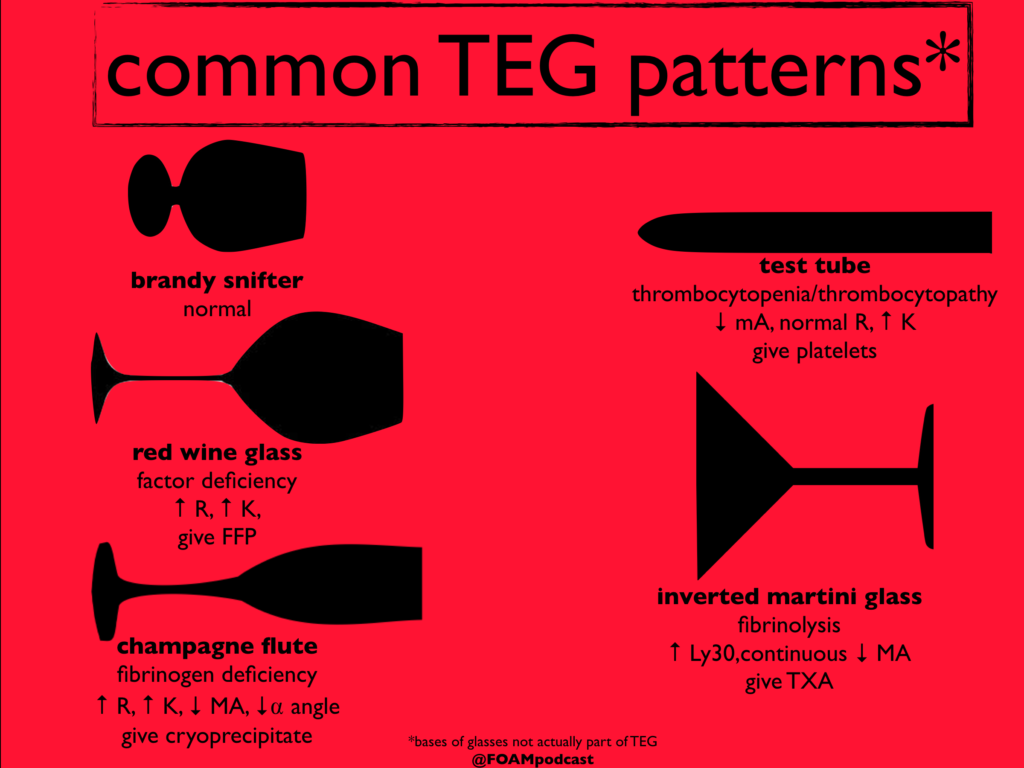
An inverted martini glass appearance on thromboelastography analysis suggests this problem, prompting administration of this medication.
Excess fibrinolysis, TXA
500
CT imaging with contrast of this oncologic disease complication may be characterized by significant venous collateral formation.

SVC syndrome.
500
Overtreatment (transfusion) of this acute sickle cell condition in children < 5 yo that presents with acute anemia and abdominal pain may cause thrombotic complications once stasis is improved.
Acute Splenic or Liver Sequestration
Cautious transfusion for HD compromise or severe symptoms related to acute anemia, NOT to normalize the Hgb level. Target Hgb 8-10.
500
TRALI is characterized by this specific hemodynamic parameter remaining normal or low in comparison to TACO
PCWP or CVP
TRALI (Transfusion-Related Acute Lung Injury) and TACO (Transfusion-Associated Circulatory Overload) are both severe, acute respiratory complications occurring within 6 hours of a blood transfusion, characterized by pulmonary edema. TRALI is a non-cardiogenic, immune-mediated reaction causing lung inflammation, whereas TACO is a cardiogenic, hydrostatic reaction caused by fluid overload