Too little too late
Too much of nothing
Clots and what not
Keep bleeding
Miscellaneous
100
36 y/o woman w/ PMH of hyperthyroidism who comes in w/ complaints of fatigue for several months. CBC revealed pancytopenia. BMBx showed the following: Dx?
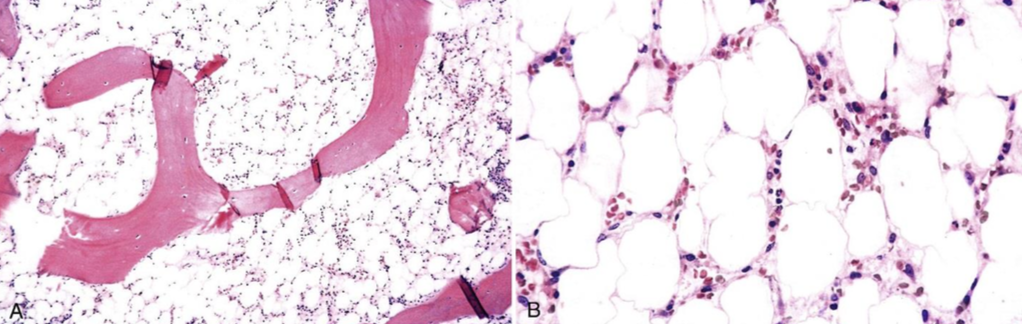
Aplastic anemia
hypocellular bone marrow

100
Initial treatment for acute promyelocytic leukemia?
All-trans retinoic acid (ATRA)
APL is a subset of AML w/ cytogenic t(15;17).
100
Alternative anticoagulant for patients suspected of HIT?
Argatroban, bivalirudin.
Screening test w/ ELISA
Confirmatory test w/ serotonin release assay or hep-induced platelet aggregation assay.
100
Young, healthy female w/ a hx of menorrhagia comes in w/ cc of fatigue and dyspnea. Routine lab show the following:
Hgb: 10
MCV: 70
RDW: Elevated
TIBC: Low
Blood smear:

Iron deficiency anemia
100
A 65 patient w/ a retroperitoneal bleed develops acute respiratory distress several hours after blood transfusion. He has a PMH of CKD stage III and CHF. EKG- sinus tachy. CXR- bilateral opacities. Vitals are wnl and he is afebrile. What is the most likely diagnosis?
TACO (transfusion-associated circulatory overload)
Treat w/ diuretics, slower rate.
200
30 y/o AAF w/ PMH of sickle cell disease came in w/ cc of chills, fatigue and dyspnea. She think she caught the same virus as her toddler who was sick a couple of weeks ago. Vitals and PE are wnl. CBC showed low Hgb and low retic count. All other labs are wnl. What is the leading dx?
Pure red cell aplasia
Can be primary or secondary.
BM Bx confirms diagnosis.
200
65 y/o patient presents with fatigue, weight loss, fever and chills for the past several weeks. Splenomegaly was palpated. Bone marrow was difficult to aspirate. Biopsy showed the following:
Most likely diagnosis?
Primary myelofibrosis.
-Diagnosis requires BMB showing fibrosis in the marrow and exclusion of other causes.
-Usually "dry tap"
-Only treatment is allogeneic hematopoietic stem cell transplantation.
-Ruxolitinib
200
29 y/o female came in for routine f/u. She complains of heavy menstruation cycles and nose bleeds for the past several months and also intermittent bleeding when she brushes her teeth. CBC, PT and PTT labs were all wnl. What is the most likely diagnosis?
Von Willebrand disease
Typically asymptomatic unless provoked such as w/ menstruation, surgery.
200
How to tell the difference between folate and vitamin b12 deficiency?
Folate def: Elevated homocysteine, normal MMA
Vitamin B12 def: Elevated homocysteine and MMA
200
Patient undergoing chemotherapy for AML suddenly develops a fever. Diagnosis criteria for febrile neutropenia and treatment is?
Temp >101 OR >100.4 x1 hr with ANC <500.
Empiric treatment:
Cefepime OR Zosyn OR Meropenem
Vancomycin is NOT part of initial regimen. Only consider if suspected catheter-related infection, skin or soft tissue infection, pneumonia, or hemodynamic instability.
300
The triad of Felty Syndrome
Neutropenia, splenomegaly, and rheumatoid arthritis.
Isolated neutropenia is associated with HIV, CMV, EBV, chemotherapy, autoimmune diseases.
-Mostly mild and only require treatment of the underlying disease.
-Some require granulocyte colony-stimulating factor (such as in chemo)
300
Elderly woman comes in w/ complaints of headaches, pruritus that worsens when she showers, and erythema of her face. PMH significant for TIAs and HTN. Lab work significant for hemoglobin of 18 and PLT of 500k. What is the most likely differential?
Polycythemia vera.
Diagnostic test is JAK2 V617F mutation. (97%)
Major criteria for PV
-Hgb >16.5 in men and >16 in women.
-BMB showing hypercellularity and increased reticulin and collagen fibrosis.
-Positive for JAK2 or exon 12 mutation.
300
TTP is associated with what deficiency?
ADAMTS13
300
45 y/o Caucasian male w/ PMH of HTN and DMT2 w/ recent diagnosed of non-ischemic cardiomyopathy came in w/ cc of joint pain in his hands. On PE, 2nd and 3rd MCP are swollen but have preserved ROM. You elect to obtain some initial labs and an XR which showed the following:

What is the most likely diagnosis?
Hereditary hemochromatosis
Presents w/ DM, elevated LFTs, "bronze skin", fatigue, arthralgia and "hook osteophytes on 2nd, 3rd MCP".
Initial labs: transferrin saturation and ferritin
300
A patient w/ newly diagnosed MM came in for evaluation. He is asymptomatic and denies any back pain. SPEP show an IgA protein spike of 4g/dl. Skeletal survey was negative for any lesions. What is the next appropriate test?
Whole body MRI.
The International Myeloma Working Group recommends that all patients with smoldering multiple myeloma undergo whole body MRI to assess for lytic lesions.
400
65 y/o asymptomatic male came in for routine lab work. Found to have pancytopenia. Peripheral blood smear showed dysplastic cells . Bone marrow biopsy confirmed what dx __1?
Myelodysplastic syndrome
BM Bx is diagnostic.
Main goal of MDS is to treat the cytopenia and decrease progression to AML.
400
How to diagnose CML by FISH?
Philadelphia chromosome t(9;22)
400
30 y/o female w/ no known PMH came in w/ acute dyspnea. CTA showed saddle PE and she underwent emergent mechanical thrombectomy and systemic TPA. She denies any hx of recent travel, sx, immobility but does report her grandmother has a hx of SLE. You are concern w/ ___ dx and you want to order ___labs?
Antiphospholipid syndrome
Anti-cardiolipin antibody IgG/IgM
Anti beta-2-glycoprotein 1 IgG/IgM
Lupus-anticoagulant.
400
65 y/o female w/ PMH of CKD stage III comes in for evaluation of fatigue. Her most recent Hgb is 8. What do you want to consider starting her on?
CKD with Hgb >10 and not on dialysis- no erythropoietin stimulating agents.
CKD with Hgb <10 should be consider ESA depending on transfusion frequency, symptoms
400
70 y/o male recently diagnosed w/ CML and was started on TKI for initial treatment. During his f/u, what is the main side effect of TKIs you should be aware of?
Prolongation of QTc.
Routine evaluation w/ EKGs are required.
500
65 y/o asymptomatic male came in for routine lab work. Found to have pancytopenia. Peripheral blood smear showed dysplastic cells . Bone marrow biopsy confirmed MDS. Cytogenetics showed a -5q abnormality. Which DOC can be use for this subset of patients?
Lenalidomide
Patient's with the -5q cytogenetic abnormality of low-risk MDS can be treated with lenalidomide.
500
Name the causes of eosinophilia (minimum of 3)
CHINA
Collagen vascular diseases, Helminthic infections, Idiopathic hypereosinophilic syndrome, Neoplasia, Allergy.
500
Pentad of TTP?
Fever Anemia Thrombocytopenia Renal Neuro
Triggered by drugs or inherited.
Treatment is FFP, plasma exchange daily, steroids.
If refractory, consider adding rituximab.
500
Antibodies associated w/ warm autoimmune hemolytic anemia and cold agglutin disease?
IgG in warm
IgM in cold
500
Which stage of colon cancer would benefit most from adjunctive chemotherapy?
Stage III.
Stage II- resection.
Stage II w/ high risk factor- 5FU or capecitabine