No Brain, No Gain
Skin in the Game
Matters of the Heart
Breath of Fresh Air
Urine Trouble
Exposure Therapy
Poo-pourri
100
This is the likely causative organism in a patient with fever, headache, altered mental status and these T2-weighted MRI findings. 
Herpes simplex virus-1
Notes:
- Dx w/ HSV PCR of the CSF
- Tx w/ high-dose IV acyclovir for 2-3 weeks
100
Limited cases of this superficial staphylococcal infection can be managed with this treatment

Topical mupirocin
100
This is the recommended initial imaging test for a patient with fever, a heart murmur, and these physical exam finding:
TTE
TEE recommended if:
- suspected IE and nondiagnostic TTE
- complications have developed or are clinically suspected
- intracardiac devices or leads are present
100
Provide an antibiotic you could use for empiric outpatient treatment of community acquired pneumonia in a healthy adult without MRSA or Pseudomonas risk factors
Amoxicillin
OR
Doxycycline
OR
Macrolide (if local pneumococcal resistant <25%)
100
Provide an antibiotic regimen (agent and duration) for a non-pregnant patient with uncomplicated cystitis
1. 3 days of TMP-SMX
2. 5 days of nitrofurantoin
3. Single-dose of fosfomycin
100
Criteria for tuberculin skin test positivity in a healthcare worker
10 or more mm of induration
Notes:
- 5 mm: threshold for pts w/ HIV, close contacts of people with active TB, organ transplant recipients, immunosuppressed patients, people with CXR findings c/w prior TB infection
- 10 mm: threshold for recent arrivals from high-prevalence countries, people w/ SUD, residents or employees of high-risk congregate setting, mycobacteriology lab personnel, people with high-risk comorbidities
- 15 mm: threshold for those with no TB risk factors
100
Management of watery diarrhea in a traveler without fever/systemic illness if symptoms restrict activity
Azithromycin
Fluoroquinolone (eg, ciprofloxacin) acceptable, but beware of increasing resistance
Note:
- Travelers diarrhea caused by ETEC is usually self-limiting and can be managed with supportive care
200
What are the two most common organisms causing community-acquired bacterial meningitis in adults?
1. Streptococcus pneumoniae
2. Neisseria meningitidis
Note: Listeria monocytogenes not a top-two bacterial pathogen, but associated with bacterial meningitis in adults age > 50
200
Recommended imaging study for all new diabetic foot infections
Plain x-ray
- Assess for soft tissue gas, foreign body, and bony involvement
- Some patients (e.g., unresolving infection despite wound care and appropriate antibiotics) require MRI to assess for osteomyelitis
200
This screening is recommended in patients with endocarditis due to Streptococcus gallolyticus and Clostridium septicum
Colonoscopy
Streptococcus gallolyticus and Clostridium septicum are associated with colon cancer
200
A patient is admitted for multilobar pneumonia. He has hyponatremia and diarrhea. What is the likely causative organism and how would you diagnose it?
Legionella pneumophila, diagnosed with urine Legionella antigen
200
These are the two indications for treatment of asymptomatic bacteriuria
1. Pregnancy
2. Invasive urologic procedures
200
Following a needlestick injury, what labs should be obtained from the source patient and from the HCW?
Source pt: HBV serology, HCV Ab, and HIV
HCW: Baseline HIV, HCV Ab w/ reflex to HCV RNA
(HBV immune status of HCW should ideally be known prior to exposure)
200
Likely infectious pathogen and recommended treatment for a patient who develops greasy, foul-smelling diarrhea after drinking from a fresh water stream.
DOUBLE-OR-NOTHING: Giardiasis is associated with this primary immunodeficiency
Giardia lamblia
Tx with metronidazole (or tinidazole or nitazoxanide)
DOUBLE-OR-NOTHING: Selective IgA deficiency
300
What is the empiric antibiotic regimen for community-acquired bacterial meningitis in a patient >50 years of age?
DOUBLE-OR-NOTHING: For which bacterial pathogen does adjunctive dexamethasone have the strongest evidence for reducing morbidity and mortality?
IV ampicillin (Listeria coverage) plus
IV ceftriaxone or cefotaxime plus
IV vancomycin
DOUBLE-OR-NOTHING: Adjunctive dexamethasone for S. pneumoniae meningitis
Note for beta-lactam allergy: may use IV moxifloxacin instead of cephalosporin, IV TMP-SMX instead of ampicillin
Note for health care-associated bacterial meningitis: Tx w/ vancomycin plus ceftazidime, cefepime, or meropenem
300
This is the preferred method of identifying the causative organism of a diabetic foot infection
Culture of deep tissue curettage/biopsy
Note:
- Superficial wound culture are typically polymicrobial and reflect colonization
300
Agent and duration of treatment for early disseminated Lyme disease with severe, symptomatic PR prolongation
Ceftriaxone for 14-21 days
(Transition to oral doxycycline once improving, complete 14-21 total days of therapy)
300
Anaerobic coverage in the treatment of community acquired pneumonia is required only if one of these two conditions are present (need to provide both conditions).
1. Empyema
2. Lung abscess
300
Recommended next step for a patient being treated for pyelonephritis with persistent fever after 72 hours
US or CT to assess for perinephric abscess or evidence of obstruction
300
A HCW is exposed to blood from a patient with HIV in a needlestick injury. Baseline HIV testing for the HCW is negative. If post-exposure prophylaxis is considered, what's the latest it can be started?
No more than 72 hrs
300
Define severe C. difficile infection
C. diff infection with at least one of the following:
- leukocyte count at least 15K/uL
- serum Cr at least 1.5 mg/dL
Nonsevere C. diff infection may be managed with PO metronidazole if neither oral fidaxomicin nor vancomycin are available (or both are contraindicated)
400
A patient presents with fever, nuchal rigidity, and photophobia. List at least 3 indications to get a CT head before proceeding with lumbar puncture.
1. Papilledema
2. Focal neurologic deficits
3. Altered mental status
4. H/o CNS disease (mass lesion, stroke, or focal infection)
5. Immunocompromise (eg, HIV, immunosuppressive therapy, solid organ or HSC transplantation)
6. New-onset seizures
Note:
- CSF sample should be sent for Gram stain, culture, and PCR before antibiotics initiation
- Additionally, get CSF cell count, glucose, and protein
- Bacterial meningitis: low (<40 mg/dL) glucose
400
This is the primary treatment for treatment of any purulent SSTI of any severity.
DOUBLE-OR-NOTHING: List at least 4 oral antibiotic options for empiric MRSA SSTI treatment
Incision and drainage
DOUBLE-OR-NOTHING:
1. TMP-SMX
2. Doxycycline
3. Minocycline
4. Clindamycin (beware of emerging resistance)
5. Linezolid
6. Delafloxacin
400
List 3 possible indications for surgery in the management of infective endocarditis.
- Valvular dysfunction associated with acute HF
- Fungal infection, or highly resistant organisms
- Large (> 10 mm) vegetations, particularly on the mitral valve (higher risk for embolization)
- Heart block
- Annular or aortic abscess
- Recurrent systemic embolization on antibiotic therapy
- Prosthetic valve endocarditis with relapsing infection or dehiscence
- S. aureus prosthetic valve endocarditis
400
Provide two potential antibiotic options for monotherapy of hospital-acquired pneumonia with no risk factors for antibiotic resistance.
DOUBLE-OR-NOTHING: Define hospital-acquired pneumonia and ventilator-associated pneumonia
Monotherapy regimens for HAP w/o resistance risk factors:
- Cefepime
- Pip-tazo
- Levofloxacin
DOUBLE-OR-NOTHING:
HAP = pneumonia that occurs at least 48 hrs after admission
VAP = pneumonia that occurs >48 hrs after endotracheal intubation
400
Management of asymptomatic candiduria in a patient with an indwelling urinary catheter
Removal the catheter
Antifungal therapy not warranted
400
A HCW is exposed to a patient's blood in a needlestick injury. The HCW reports receiving his HBV vaccine. How can you determine whether he is a vaccine responder?
Anti-HBs titer at least 10 mU/mL
(Ok if you don't know the seroprotective threshold, but answer must include quantitative titer. Qualitative test for HBsAb insufficient.)
400
Treatment of fulminant C. diff infection
Oral vancomycin plus IV metronidazole
Not required for points, but consider vancomycin enemas and assess for surgical indications
500
A patient presents in August with fever, altered mental status, and acute asymmetric flaccid paralysis. You suspect the most common arboviral cause of encephalitis in the US, so you'll need obtain this laboratory test.
West Nile Virus IgM in the CSF
Note on WNV:
- Occurs in the US in summer and fall
- More severe presentations occur in elderly patients, immunocompromised, and transplant recipients
- May present with encephalopathy, meningitis, acute asymmetric flaccid paralysis (may mimic polio)
- CSF PCR is insensitive for neuroinvasive WNV and IgM antibody testing is preferred
500
Provide an empiric antibiotic regimen you would use to treat this: 
Empiric tx of necrotizing fasciitis:
1. Vancomycin or daptomycin plus
2. Pip-tazo or carbapenem
Note: clindamycin or linezolid recommended by some experts for suppression of toxin production
500
List 3 indications for prophylactic amoxicillin before invasive dental instrumentation.
DOUBLE-OR-NOTHING: List all 5 minor Duke criteria for infective endocarditis
- Previous, relapsed, or recurrent IE
- Prosthetic heart valve/material
- LVAD
- Heart transplant with valvulopathy
- Unrepaired cyanotic congenital heart disease
- Repaired congenital heart disease w/ residual defect at the site or adjacent to the site of a prosthetic patch/device
DOUBLE-OR-NOTHING:
Duke minor criteria:
- predisposing heart condition or IVDU
- fever
- vascular phenomena
- immunologic phenomena
- microbiological evidence not meeting a major criterion
500
What test is most likely to identify the causative organism in a patient with subacute cough >4 weeks in duration with posttussive emesis?
Serology for Bordetella pertussis IgG
Note:
- Nasopharyngeal swab for Bordetella pertussis culture or PCR useful if early (<4 weeks duration); sensitivity drops after that
500
What is the treatment for a patient with urethritis and a positive urine NAAT for Neisseria gonorrhoeae. NAAT for Chlamydia trachomatis was not performed.
DOUBLE-OR-NOTHING: Which infection (Gonorrhea or Chlamydia trachomatis) AND site of infection warrants testing for cure in nonpregnant patients?
Parenteral ceftriaxone plus oral doxycycline (preferred) or oral azithromycin (if pregnant)
DOUBLE-OR-NOTHING: Pharyngeal gonorrhea warrants test of cure with NAAT and culture 2 weeks after therapy. Test of cure unnecessary in uncomplicated urogenital or rectal infection.
Note: Testing for reinfection after 3 months is warranted for both gonorrhea and Chlamydia trachomatis infection
500
A HCW is exposed to a patient's blood in a needlestick injury. HBV serologic testing is performed on the source patient. Interpret the findings:
- HBsAg positive (+)
- HBsAb negative (-)
- HBc IgG positive (+)
- HBeAg positive (+)
- HBeAb negative (-)
- ALT high
- HBV DNA 30K IU/mL
DOUBLE-OR-NOTHING: Should the patient be treated for HBV infection?
Immune active chronic HBV infection
DOUBLE-OR-NOTHING: Yes, treat
Indications for HBV infection tx:
- acute liver failure
- cirrhosis
- immune active phase or reactivation phase of chronic HBV infection
- 3rd trimester of pregnancy with viral load >200K IU/mL
500
Management of a patient with bloody diarrhea, AKI, thrombocytopenia, and the following peripheral blood smear findings: 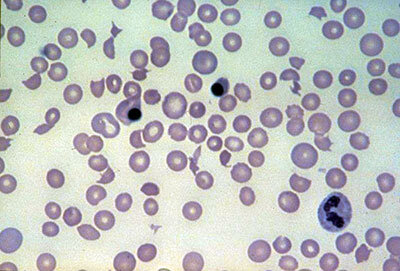
Supportive care
Enterohemorrhagic E. coli infection:
- caused by Shiga toxin-producing strains of E. coli (most commonly O157:H7)
- causes bloody diarrhea with associated hemolytic uremic syndrome (triad of MAHA, thrombocytopenia, and AKI)
- typically no fever, distinguishing it from other causes of bloody diarrhea
- antibiotics not beneficial and increase the risk of HUS