Breaking Bad (Drugz)
28 Days Later (Bugz)
The Perfect Score (Tests)
House (Clinical)
Rear Window (Imaging/ Histopath)
100
First line for IIM-ILD besides steroids (can accept any 4 answers)
What are MMF, AZA, TAK (calcineurin inhibitor), or RTX?
-MMF works really well for SS especially she said
-tocilizumab/ Actemra IL-6 is mainly for SS-ILD although RA in general might use it
-more data for TAK in other countries but is non-inferior in a study in the US comparing; TAK actually did slightly better than MMF and AZA but the pt population was younger and earlier disease
-AZA technically non-inferior to MMF statistically but had more non-statistically significant deaths- mirrors SLE study but SLE had more power so was statistically significant
-don't give steroids to SS pts usually unless after lung transplant- then can consider bc usually far into dz course so have less risk she said
100
common reason to use antibiotics/ hospitalize in ILD mentioned in the video
what is dysphagia/ aspiration?
100
part of the cell affected in myositis antibodies
what is cytoplasm?
-SSA, IIM antibodies, antiphospholipid antibodies
100
Lung limited MDA5 dermatomyositis/myositis prognosis
What is worse/bad/severe?
3 phenotypes of MDA5
1) female predominant w/ skin, almost no ild
2) vasculitis w/ raynaud's, palmar papules- 76% survival at 36 months, worse survival than most cancers per the video
3) ILD- 20% survival at 3 months, worst, HIGHLY fatal, associated w/ rapidly progressive ILD- pneumomediastinum is common and poor prognosis
100
MC Rheumatoid arthritis ILD pattern
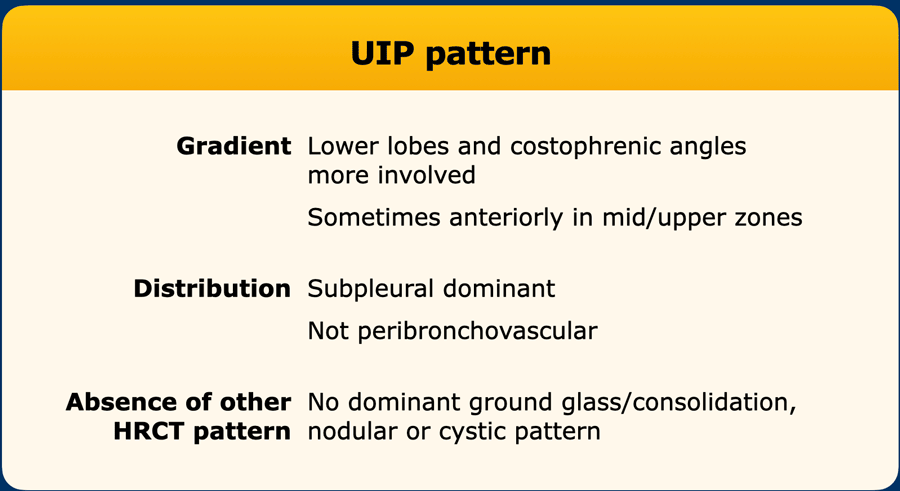
What is UIP?
Usual interstitial pneumonia- although the video said it can be 50-50 w/ NSIP (nonspecific interstitial pneumonia)
Idiopathic pulm fibrosis can also be UIP
200
mycophenolate and Nintedanib common side effect
What is diarrhea?
Synergistic in terms of efficacy but no increased rate of the SE by using both
200
viral infection should you be worried about with tacrolimus in the video
What is COVID-19?
in the video- said to give molnupiravir
200
Basic screening tests (2) for ILD in a patient with RA CCP+, long smoking hx
What is Chest CT and PFTs?
low dose ct screen- 50 to 80 years who have a 20 pack-year smoking history and currently smoke or have quit within the past 15 years
unlike scleroderma we don't necessarily test for ild in every ra ccp+ pt yet per guidelines but it is something to consider
200
Definition of rapidly progressive ILD
What is progression over weeks to months- room air to intubation/ high O2 needs?
high chance for MDA5 to progress to RP-ILD in 3 months w/ either imaging or physiology
63% of MDA5 dermato progress to RP-ILD
44% of Asys progress to RP-ILD
200
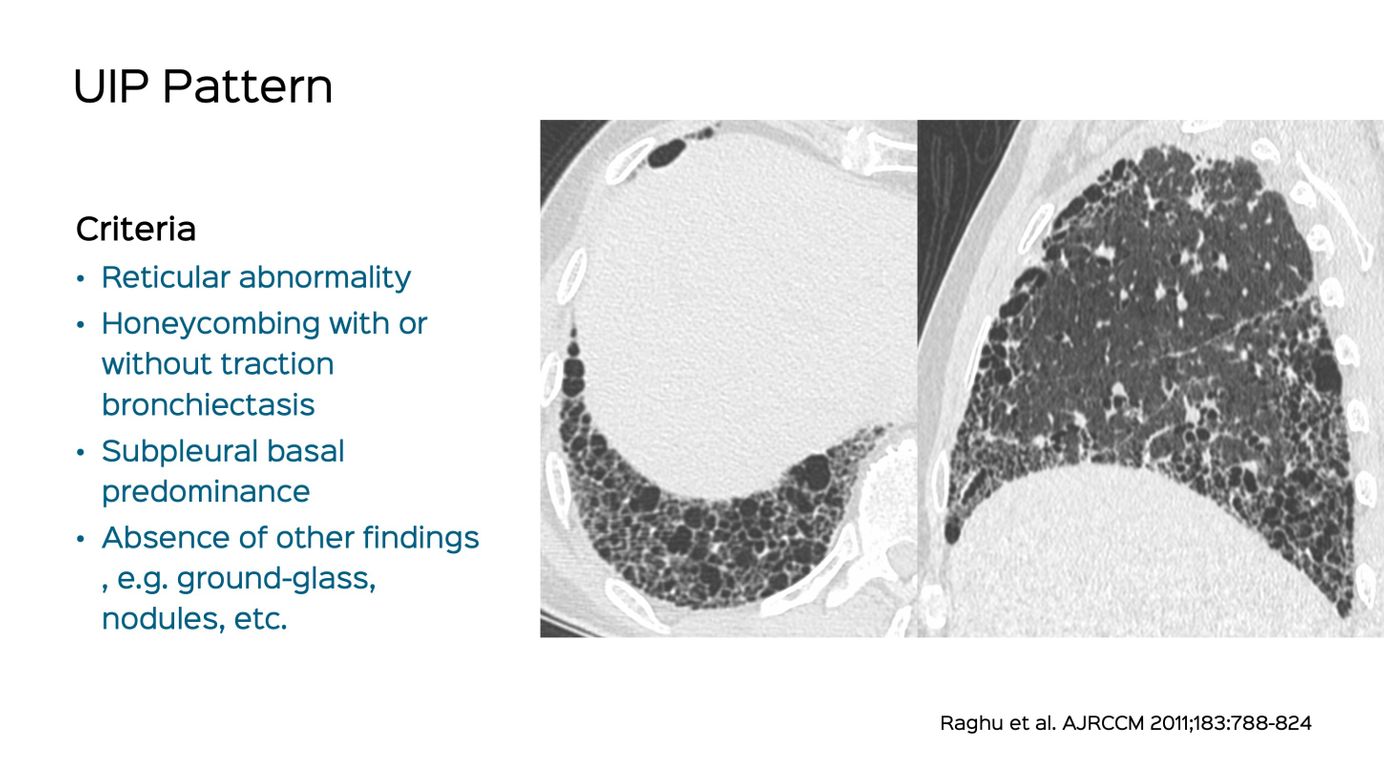
MC UIP finding
What is honeycombing?
cystic lung changes, budding of pleura
only lung pattern with good correlation of biopsy per the video
300
Good adjunct (2 acceptable answers) besides your typical immunosuppressant in SARD-ILD
What is IVIG or nintedanib?
nintedanib anti-fibrotic, more in pulm fibrosis
IVIG improves survival in dermato ILD- Secrets says fc portion of IVIG binds to C3b and C4b-> decreased complement activation
-other anti-fibrotic options nerandomilast, pirfenidone but more in IPF
PLEX is for salvage therapy but not as good data
-additional is tadalafil/PDE-5 inhibitor/bosentan/CCB for Raynaud's/ulcerations specifically

300
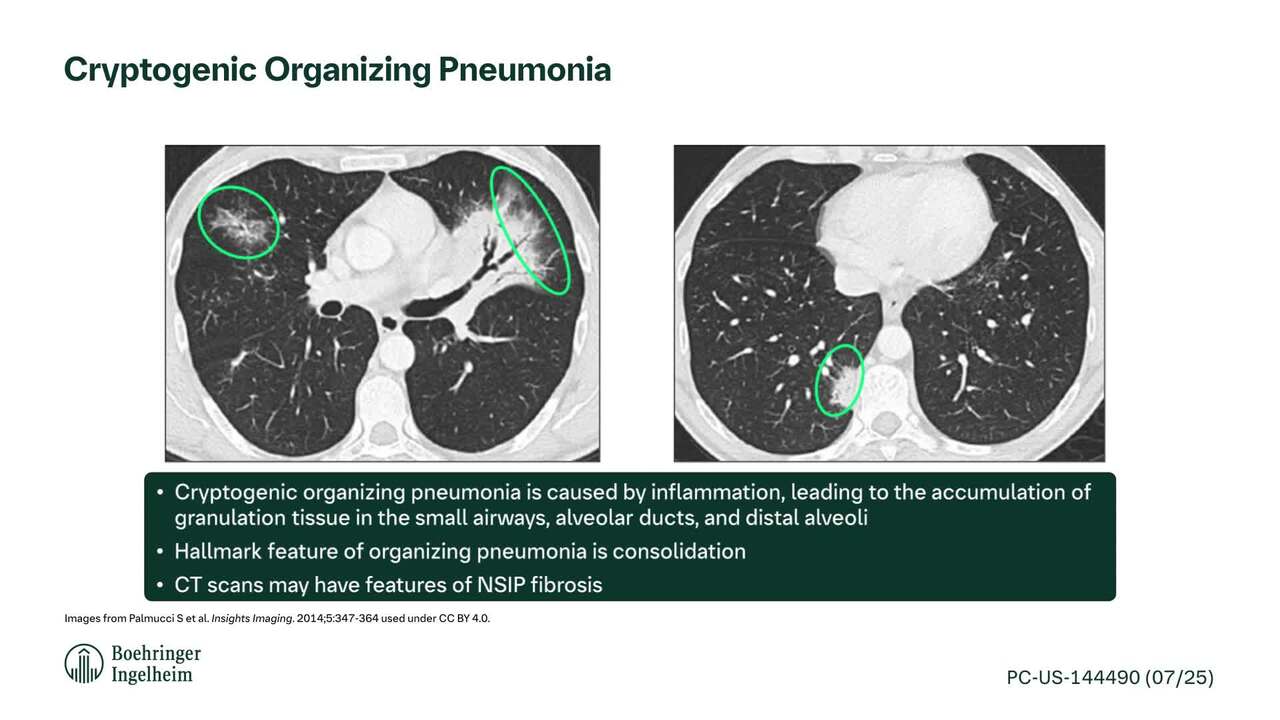
Organizing pneumonia vs fungal disease on CT per the video
What is focal consolidation (central clearing with rim of dark ground glass) vs halo sign (ground glass inside the central area)?
causes of OP various- cryptogenic (idiopathic), infxn, exposure, aspiration, autoimmune

300
reason to use 6 minute walk test (2 acceptable answers)
What is pulmonary HTN or oxygen desaturation?
ECHO is more useful for pulm HTN screening though- confirmatory is RHC
ILD destroys alveolar capillary bed increasing background pulmonary pressure
Not useful as ILD screening by itself however; people who desat are already likely to be fairly compromised per the video
300
Differential consideration besides Sjogren's with SSA/Ro52 (3 possible answers)
What are Anti-synthetase syndrome (ASys), ILD, or IIM?
20% iim associated ild per secrets
interferon inducible protein in the cytoplasm; this is in contrast to 60 which binds to small noncoding rnas in the nucleus
can be associated with MDA5 dermato as well
300
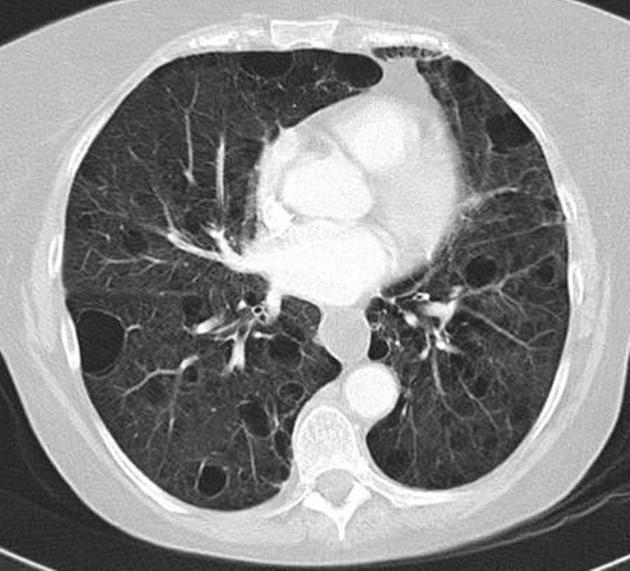
MC NSIP finding
What is ground glass?
Seen in CTD, exposure e.g. pneumoconiosis, drug, hypersensitivity

400
Reason mycophenolate does not work well on MDA5 dermatomyositis
What is interferon mediated?
She said in MDA5 use calcineurin or JAKi
HOWEVER, I looked this up on Open Evidence:
"the magnitude of interferon dysregulation in MDA5+ dermatomyositis overwhelms mycophenolate's anti-interferon effects. This is why combination therapy targeting multiple pathways—including JAK inhibitors that directly block interferon signaling downstream—shows superior efficacy compared to conventional immunosuppressants alone"
progression of MDA5 dermato is very aggressive
so it works but it might need to be used with another immunosuppressant such as high dose steroids or rituxan, but the caveat is that you increase mortality risk with infection due to compounded immunosuppression
400
PPX (2) for JAK inhibitor
What are anti-viral and Bactrim/TMP-SMX?
In RA-ILD or IIM-ILD
CMV per the studies was common, PJP- she said valacyclovir which is more for herpes but for CMV you would use valganciclovir or gangiclovir
Should also get Shingles vaccine before starting according to Secrets
400
Strong ACR recommendation against in testing for ILD
What is surgical lung biopsy?
risk of early mortality in SARD-ILD is low and benefit does not outweigh risks in this case
2016 2% mortality in 30 days per the vid after outpatient elective surgical biopsy; 6% mortality SARD ILD in 30 days, in-patient 16% mortality in 30 days; without biopsy usually not 6% mortality in the next year so not worth the risk
400
Severe ILD/ exacerbation definition (2 possible criteria)
What is hospitalization or hypoxemia?
try to refer to lung transplant early out-patient, hopefully before they get to the point of going to the hospital
400
UIP histopathology
What are areas of scar next to areas of normal lung?
 a) NSIP- blue dots around, thick, uniform alveoli
a) NSIP- blue dots around, thick, uniform alveoli
b) Organizing Pneumonia- granulation tissue/healing in the airway
c) UIP- normal lung w/ fibroblastic foci next to areas of scar ***
d) LIP- lymphocytic aggregates
500
Should not use MTX in this case (2 scenarios) for patient with RA-ILD
What is baseline O2 with mod-severe ILD?
Speaker recommended using MTX otherwise- she felt pneumonitis risk is generally low and there are benefits to controlling RA overall inflammation for prognosis
500
ILD associated with HIV
What is LIP or Lymphocytic interstitial pneumonia?
thin walled cysts but otherwise spared
Also in Sjogren's- MC women than men
Mostly adults but if in children can be indicative of AIDS
benign lymphoproliferative disorder characterized histologically by diffuse interstitial and alveolar infiltration with polyclonal lymphocytes and plasma cells
80% of patients polyclonal or IgM monoclonal gammopathy is found
MC
ground-glass opacity (main finding) 17
interstitial thickening (~50%) 17
lower-zone predominant bilateral reticular opacification
chronic bilateral airspace opacification
Later stage can become honeycomb
5% become lymphoma
https://radiopaedia.org/articles/lymphoid-interstitial-pneumonia
500
antibodies to test for in an ILD patient with fever (multiple corrects, 2 categories)
What are MDA5 (dermato) or antisynthetase MSA's (Jo1, PL7, PL12, EJ, OJ)?
Per video + Secrets
500
Specific skin findings (2) of MDA5-dermatomyositis mentioned in the video
What are palmar papules and ulcerations (of gottron's papules)?
-others per secrets- Raynaud, heliotrope rash, v sign, shawl sign, holster sign, periungual erythema, scalp, photosensitivity, calcifications/calcinosis, hypo/hyperpigmentation in UV exposed areas (poikiloderma)
500
Name the types of ILD based on images in correct order

What are a) OP, b) NSIP, c) UIP, d) LIP?
a) OP- rim of dark ground glass, consolidative change
b) NSIP- not a lot of scar, reticular changes, grand glass
c) UIP- honeycomb- areas of ground glass only in areas of reticulation (confused w/ fibrosing NSIP)- good correlation w/ lung biopsy
d) LIP
