Pressure Injury Staging
Wound Healing
Ostomies
Nursing Interventions
If you didn't chart it, it didn't happen
100
Patient is lying supine on the bed, name three (3) high risk areas for pressure injury formation.
What are heels, sacrum, spine, elbows, scapulae, and back of head?
100
Name 4 factors that impede wound healing.
What is poor nutrition, poor blood supply, wound care, chronic conditions, age, medications, and smoking?
100
This ostomy diverts stool from the ileum.
What is an Ileostomy?
100
This intervention should be done every 2 hours to prevent pressure injuries and is a deligatable task.
(DAILY DOUBLE!!)
What is repositioning/turning?
100
This communication framework is used in the healthcare field to maintain effective communication through shift / hand off.
What is SBAR?
200
Identify this pressure injury

What is Stage 3 Pressure Injury?
200
Name 3 common wound drains.
(DAILY DOUBLE!!)
What is a penrose drain, JP drain, and Hemovac?
Woundvac works too!
200
Name three (3) purposes of ostomies
What is diversion of bodily waste, management of chronic diseases, and temporary or permanent bypass.
200
After emptying a JP drain, the nurse must do this to maintain suction.
What is compress the bulb?
200
These three measurements must always be documented for wounds.
What are length, width, and depth in centimeters?
300
Name three (3) risk factors for pressure injury formation in older adults
What is impaired sensory perception, impaired mobility, alteration of LOCs, shear and friction, pressure duration and tissue tolerance, aging, hydration status, low BP, poor nutrition, systemic factors, medical devices, chronic conditions, age related changes, moisture, and incontinence?
300
Describe the main difference between primary and secondary intention wound healing.
What is "Primary intention is where wound edges are clean and directly approximated through surgical incisions AND secondary intention is where wounds are left open to heal naturally"?
300
A healthy stoma should appear this color and texture.
What is pink/red and moist?
300
Name 3 assessments for a patient with impaired skin integrity.
What is patient history, wound assessment, circulation and sensation, risk assessment, nutritional assessment, infection assessment, and psycho-social assessment?
300
This type of drainage is thick, yellow, green, tan, or brown.
(DAILY DOUBLE!!)
What is Purulent?
(NOT PUS)
400
Identify this pressure injury
(DAILY DOUBLE!!)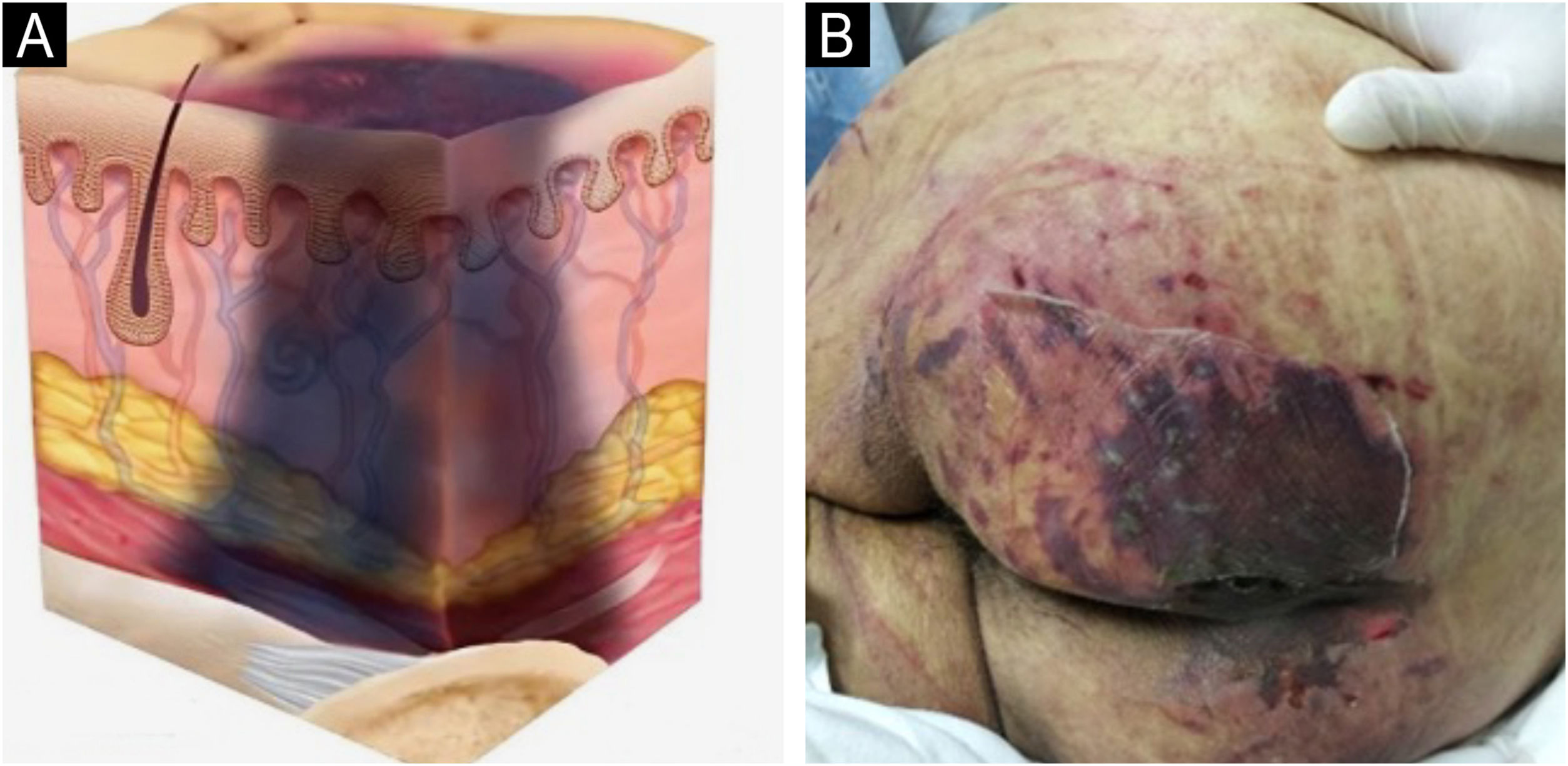
What is a Deep Tissue Injury?
400
New tissue formation involving collagen, deposition, and angiogenesis.
What is the Proliferative phase of normal wound healing?
400
This is the priority complication to monitor in ileostomy patients.
What is dehydration/electrolyte imbalance?
400
Describe how you would prep a patient with impaired skin integrity for a physical exam. Name at least 3 methods.
What is gathering subjective/objective data, building patient rapport, asking permission, maintaining patient modesty, asking patient if they want to see the assessment area, asking the patient to remove all clothing and jewelry, ensuring privacy, maintaining comfortable room temperature, explaining the assessments and answering any questions, and be aware of possible cultural concerns?
400
It is critical to do an initial skin assessment for new patients, documenting both abnormal and normal findings, because it is...
What is establishing a baseline?
500
The Braden Scale measures... (name four)
What is moisture, sensory perception, activity, mobility, nutrition, friction, and shear?
500
Name 3 factors that promote wound healing. Be specific.
What is adequate protein, vitamins A and C, zinc, good circulation, clean moist wound environment, absence of chronic diseases, younger age, healthy immune function, few to no interferences from medications, and non-smoker?
500
Name a key precaution for urostomies.
(DAILY DOUBLE!!)
What is infection monitoring due to the presence of urine?
500
Name 3 age-friendly considerations for a patient with impaired skin integrity.
What is decreased perspiration, decreased flexibility and mobility, INCREASED RISK FOR PRESSURE INJURIES, AGE-RELATED SKIN LESIONS, dry and pale skin, and decreased skin turgor?
500
Part of the assessment of a patient with impaired integrity is assessing for infection processes, name one (1) local sign and one (1) systemic sign you would monitor and document..
What is local signs: erythema, swelling, discharge, odor and systemic signs: fever, elevated WBCs, and sepsis indicators?