Terminology 1
Acronyms & Abbreviations
Assessment
Diseases, Disorders, Conditions
Terminology 2
100
What does blanchable mean?
When a (red) area of the skin is pressed, the skin turns white then returns to either red/pink/original color.
100
ABX is the abbreviation for what?
Antibiotics
100
When assessing skin turgor, when the skin does not snap back quickly (< 3 sec), what is this called?
Tenting
100
A patient presents with a skin infection caused by streptococcus pyogenes. The patient's lower leg is infected from the deep dermis to the subcutaneous fat. What skin disorder does this describe?
Cellulitis
100
What is / what does erythema mean?
Redness, reddened skin
200
What skin condition is this/what is this called?
Hives
FOR AN EXTRA 200 POINTS:
What is the medical term for hives?
200
SQ is the abbreviation for what?
Subcutaneous
200
How would you document someone's skin coloring that has no skin discolorations or issues?
Skin tone or color normal for their ethnicity
200
A wound bed appears beefy red with no slough or eschar present. This description means what/what does it signify?
Healthy granulation tissue is present
200
What does purulent mean?
Pus / yellowish or greenish fluid or exudate
300
What is eschar?
Thick, dry, black or brown layer of dead (necrotic) tissue that forms over severe wounds, burns, infections, or pressure ulcers
FOR AN EXTRA 300 POINTS:
Is a pressure ulcer with eschar stageable?
300
ID is the abbreviation for what?
Intradermal
300
What does it mean if someone is experiencing pruritis?
Their skin is itchy
300
A patient with extensive burns is most at risk for this life-threatening complication in the first 24 hours.
Fluid volume deficit
300
What is a wheal?
Raised, smooth area; can be red or paler than surrounding skin.
FOR AN EXTRA 300 POINTS:
What causes a wheal / wheals?
400
What is exudate?
Fluid from a wound, incision, etc; fluid that leaks out of blood vessels into nearby tissues.
FOR AN EXTRA 400 POINTS
Name the 4 types of exudate (points only given for all 4)
400
ABCDE is the mnemonic for what?
Asymmetry / Border (irregularity) / Color (variation) / Diameter (over 6mm) / Evolving (changing size, shape, or color)
400
What does skin integrity mean as part of the head to toe assessment?
The skin is whole and uncompromised / the overall health and completeness of the skin. It signifies skin that is undamaged, properly hydrated, and functioning effectively.
FOR AN EXTRA 400 + 400 POINTS:
How would you document no skin issues? And what factors affect skin integrity (negative factors)?
400
A patient with dark skin has a pressure injury suspected on the heel. Which assessment finding is most concerning?
A) Slight tenderness with passive motion
B) Skin turgor is < 3 seconds
C) Localized warmth and firmness
Localized warmth and firmness
400
What is the medical term for this and how would you define it?

Ecchymosis is a discoloration of the skin caused by blunt trauma or vascular issues that result from bleeding underneath
500
What is this picture indicating?
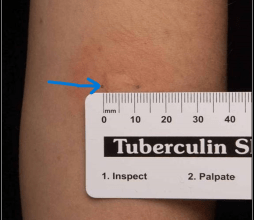
Induration
500
DTI stands for what?
Deep Tissue Injury
500
What is the Braden scale?
Tool for assessing a patient's risk of developing pressure injuries.
500
When a patient develops Stevens-Johnson syndrome from a medication reaction, the nurse should immediately discontinue the offending drug and prepare for transfer the patient to where? because the condition causes widespread epidermal necrosis similar to severe burns.
Burn unit (or intensive care unit)?
500
What is a furuncle?
A painful, pus-filled infection of a hair follicle and surrounding tissue, most commonly caused by Staphylococcus aureus bacteria