ENTfectious Disease
hEar Me Out
Ped-Files
Colonel Mustard in OR4 with a Dedo
Sleep? Never heard of it!
Saving Face
200
A patient with necrotizing fasciitis has been admitted to your service following surgical debridement by another surgical specialty. Blood and tissue cultures are growing group A strep. It is overnight and the infectious disease team is sleeping. You place orders for Zosyn and Linezolid due to your extensive knowledge of microbiology. What is your rationale for including Linezolid; what is its mechanism of action?
Linezolid has excellent coverage of group A strep (unlike other ribosome inhibitors). It functions as a 50S subunit inhibitor of bacterial ribosomes. Ribosome inhibition prevents synthesis of GAS toxins, which include:
Streptoccocal pyrogenic exotoxins (SPEs)-> Superantigens causing cytokine storm and toxic shock -> sepsis
Streptolysin O&S->Forms pores in host cells and induces necrosis
Streptokinase, hyaluronidase->Degrades connective tissue and prevents clotting allow for rapid spread of infection
200
Which part of the cochlea is the cochlear implant inserted (through what & into what space)?
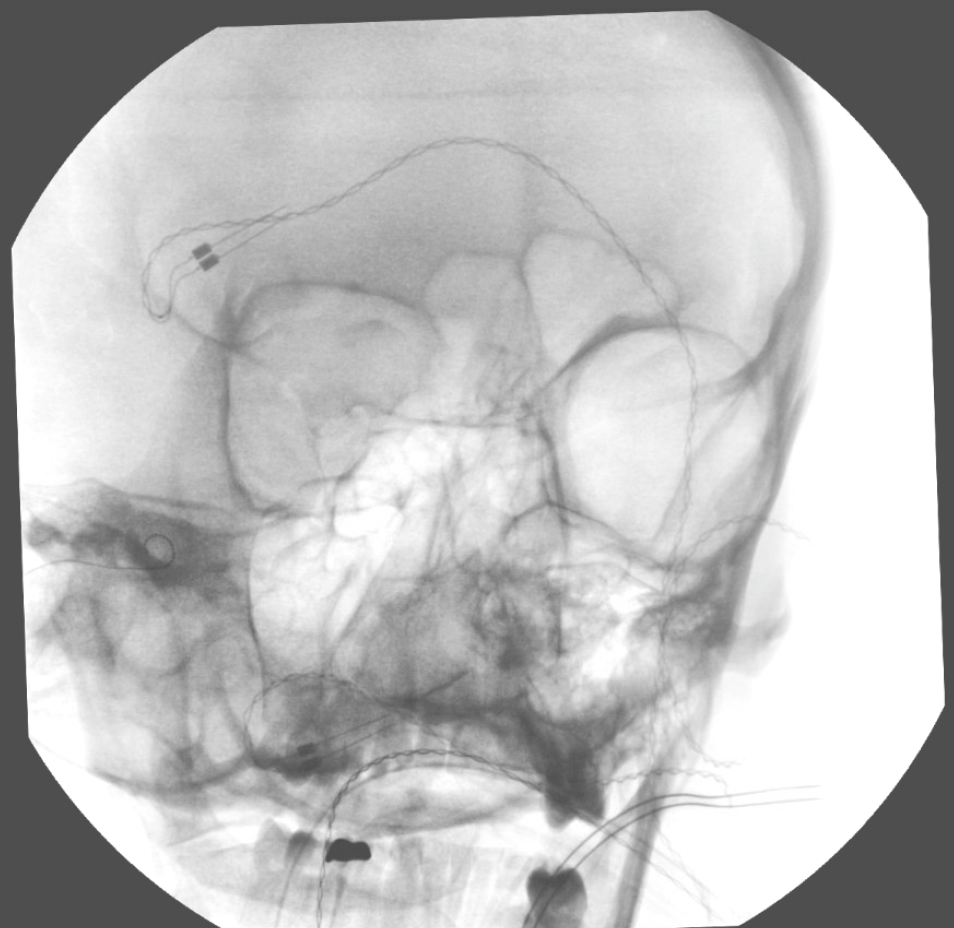
What is through the round window into the scala tympani (perilymph)?

200
A definitive diagnostic marker for this lesion & treatment?

What is GLUT-1 & Propranolol?
- Infantile Hemangioma, absent at birth, appear early infancy, proliferate rapidly durst first 6 months of life (c/w Vasc Malformations which present @ birth, enlarge proportionally w patient throughout life)
- pygoenic granulomas & vasc malformations do NOT stain positively for GLUT-1.
- propranolol 0.6mg/kg BID then 1.7 mg/kg BID.
- PHACE: Posterior fossa abnormalities, hemangiomas, Arterial abnormalities, cardiac anomalies, eye anomalies
200
What are the frequencies of KTP, Nd:YAG, Er:YAG, and CO2 lasers respectively?
What is KTP 532nm, Nd:YAG 1064nm, Er:YAG 2940nm, and CO2 10600nm
Nd: YAG: 1064 nm (neodymium-doped yttrium aluminium garnet)
- low water absorption , penetrates deeper, focusing on coagulation, vascular lesions, and collagen stimulation, often with less downtime. Deep skin tightening, vascular lesion treatment, hair removal, and acne treatment. primarily non-ablative (heats/coagulates)
Er: YAG: 2940 nm (Erbium-doped yttrium-aluminum-garnet)
- (highly absorbed by water)
- superficial, precise ablation (skin resurfacing, shallow cavity removal) with minimal thermal damage. Precision skin resurfacing, treating superficial wrinkles, moles, and dental cavities.
- primarily ablative (cuts/removes tissue).
KTP (Potassium Titanyl Phosphate): 532 nm (Hemoglobin)
CO2 laser: 10,600 nm (H2O)
200
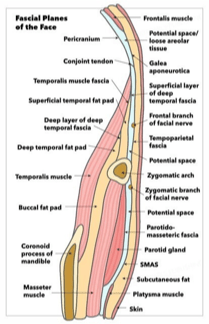
The stage at which a patient undergoing PSG is noted to have this pattern on EEG.
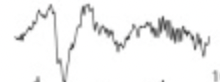
N2.
200
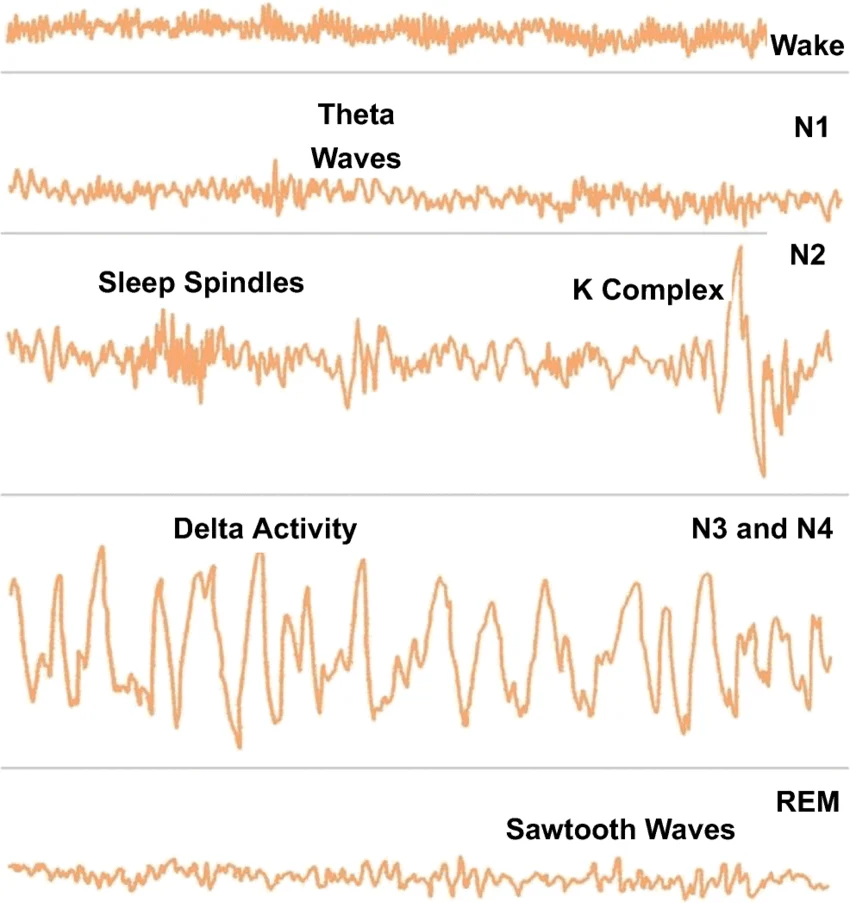
This is the fascial layer that the temporal branch of the facial nerve is located superior to the zygoma
What is just deep to the temporoparietal fascia (TEMPOROPARIETAL FASCIA = SUPERFICIAL TEMPORAL FASCIA = SMAS)
- SMAS continuous with galea and platysma
- Mimetic muscles innervated from deep except: Mentalis, levator anguli oris, buccinator
400
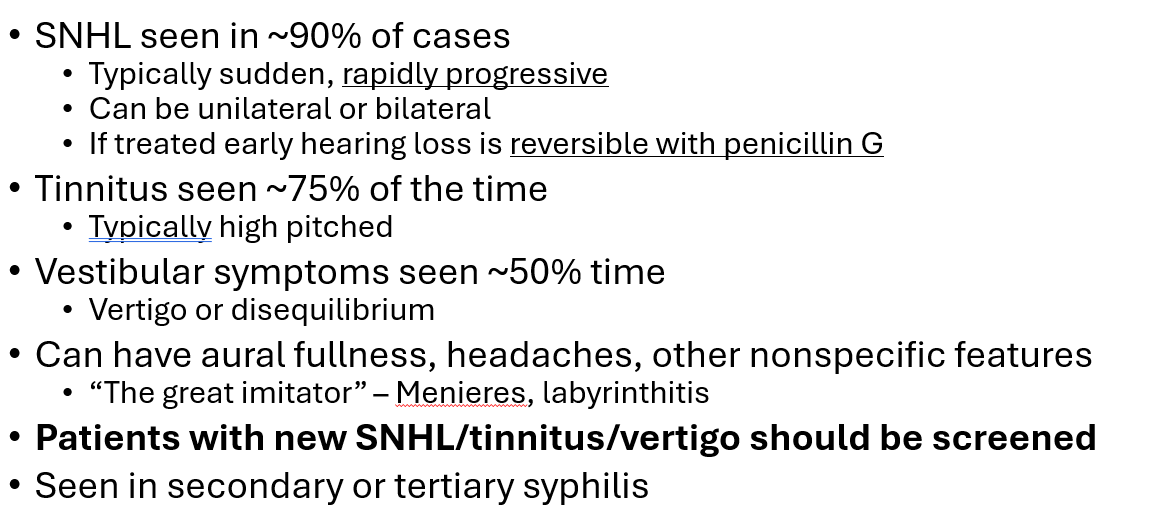
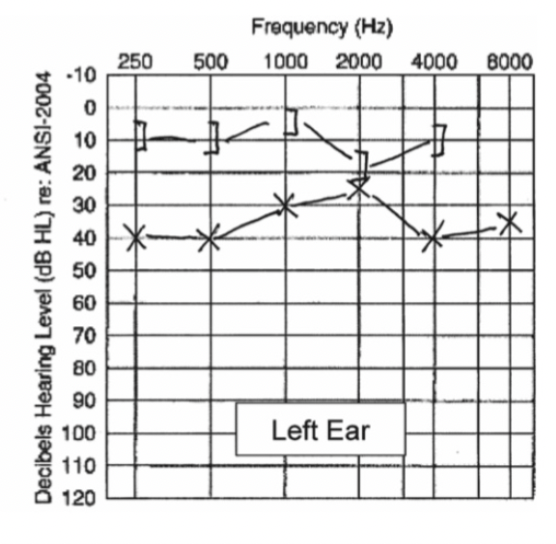
Describe the clinical features and audiogram findings of otosyphillis
400
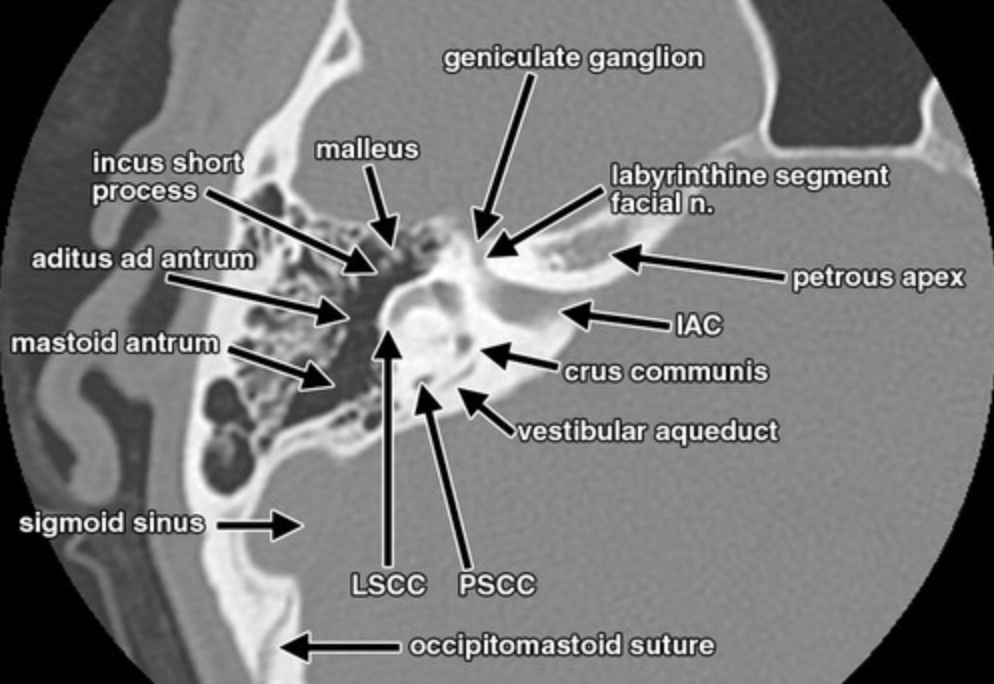
This is the most common site of facial nerve injury after temporal bone fracture.
What is the perigeniculate region?
- perigeniculate region of the facial nerve (CN VII) is the most common site of injury in temporal bone fractures. This area is located in the labyrinthine segment of the facial nerve, which curves between the vestibule and cochlea.
400
This syndrome subtype is characterized by moderate to severe sensorineural hearing loss and retinitis pigmentosa that manifests later in life, but it features unaffected vestibular function.
What is Usher Type 2?
Usher Syndrome: 1st MC AR syndromic HL, retinitis pigmentosa (tunnel vision, blindness) cataracts, +/- cognitive impairment, delayed walking.
- MC type 2 (SNHL, legally blind by mid-adult, normal vestibule.)
- Electroretinography/Ophtho eval
- Scheibe malformation: cochleosacular dysplasia. (Seen in Usher, Refsum, Down and Warderburg)
400
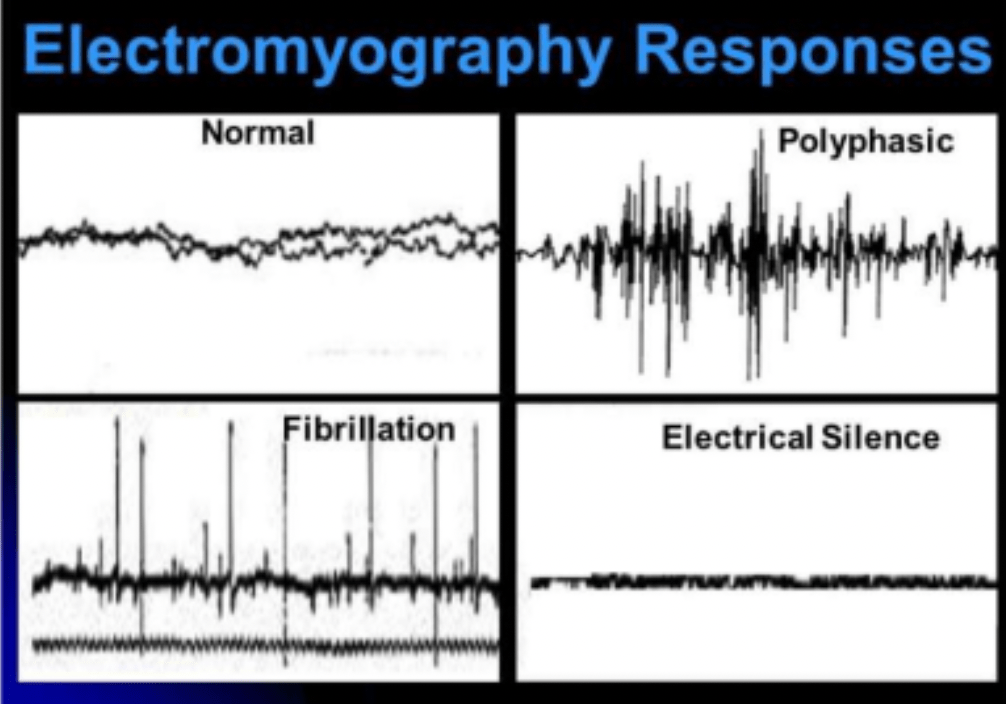
What does this EMG pattern indicate?
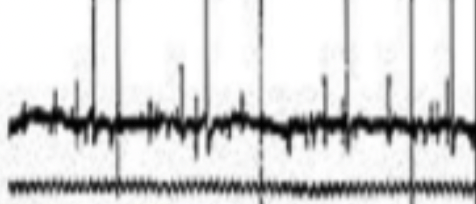
What is denervation?
Normal AP w normal recruitment
Fibrillation + spikes: denervation
Polyphasic: Reinnervation:
400
A hypopneic episode (2 definitions)
A partial reduction in airflow (≥30%) lasting ≥10 seconds, associated with 4% O2 reduction
Or
A partial reduction in airflow (≥50%) lasting ≥10 seconds, associated with 3% O2 reduction or an EEG arousal
400
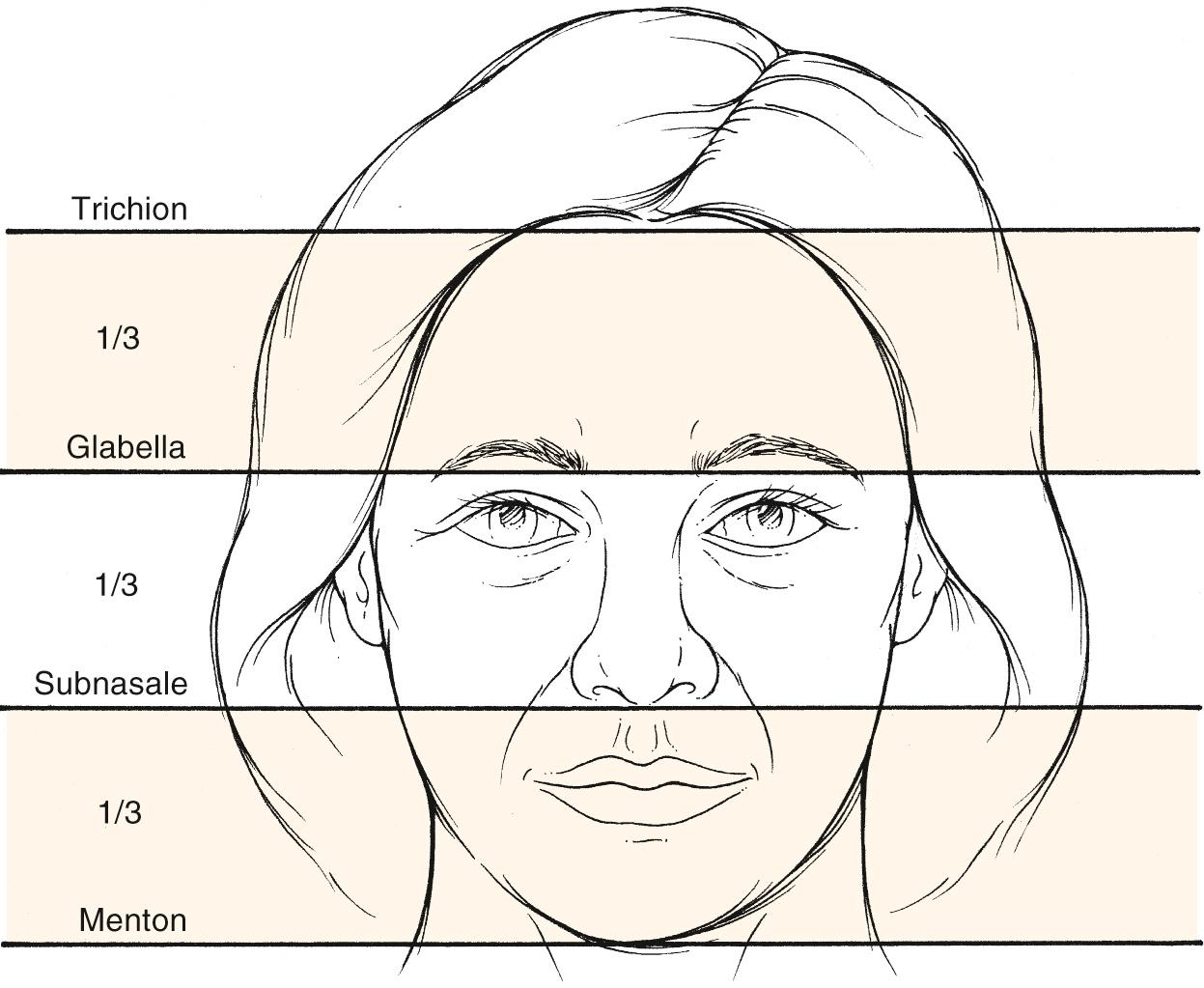
The upper third of the face is demarcated by these two structures
Trichion and glabella
600
•List 5 antibiotics with MRSA coverage (must include 5 for credit – no partial credit)
Needs >90% of strain susceptibility to be accepted
•Vancomycin
•Linezolid
•TMP-SMX
•Doxycycline
•Daptomycin
•Tigecycline
•Ceftaroline (+/- avibactam) (5th gen)
•Ceftobiprole (5th gen)
•Dalbavancin (Lipoglycopeptide with extendo release)
•Delafloxacin (only one to also provide reliable pseudomonas coverage)
•Mupirocin (count it!)
600
What is the diagnosis and 2 common audiologic findings?
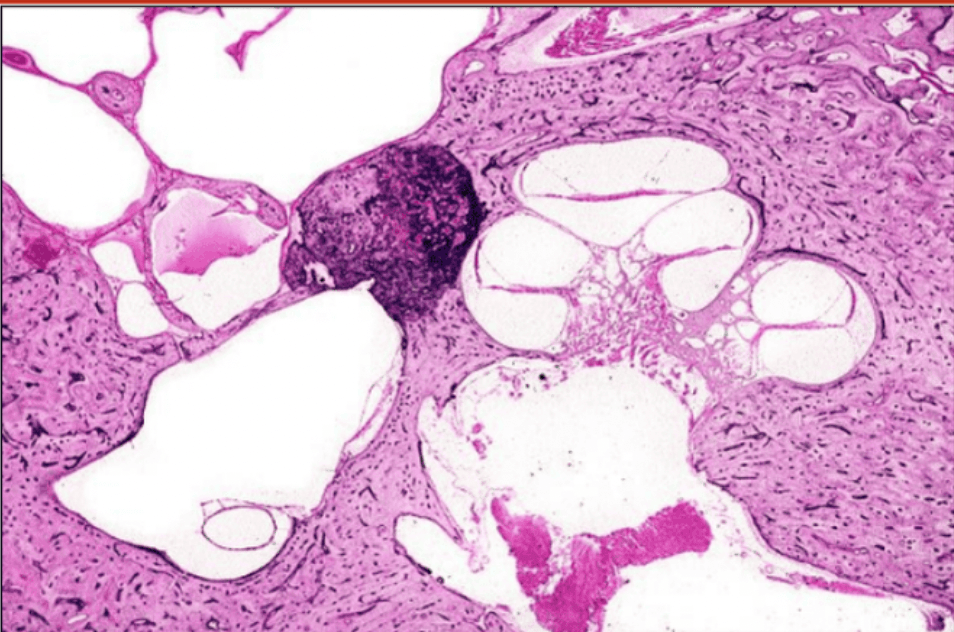
What is Otosclerosis, CHL, Carharts Notch, Absent Acoustic Reflexes?
H&E-stained section showing a solid stapedial footplate where the annular ligament has been totally replaced with otosclerosis
- Conductive hearing loss with gap closes a 2kHz Carhart's Notch. Acoustic/stapedial reflexes absent. Paracusis of Willis (hearing better when noise present in 35-50% pts). MC at anterior to the stapes footplate called the fistula ante fenestrum (2nd MC round window). otospongiosis.
600
The affected gene of an anion exchange protein responsible for an autosomal recessive form of syndromic hearing loss.
What is SLC26A4?
Iodide/Chloride exchange protein that also participates in the secretion of bicarbonate in the kidney.
Pendred syndrome: 2nd MC AR syndromic HL, SLC26A4, pendrin protein, defective iodine metabolism/organification. (anion exchange: chloride/iodide transporter; Cl/HCO3-- bicarbonate secretion in kidney)
- SNHL, normal middle/outer ear, +/- b/l mondini deformity w enlarged vestibular aqueduct, variable vestibular fx.
- Child with Euthyroid goiter
- Perchlorate test is positive.
Iodide/Chloride exchange protein that also participates in the secretion of bicarbonate in the kidney.
600
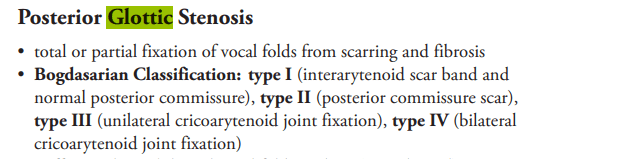
What is the classification for posterior glottic stenosis with a posterior commissure scar band?
what is bodgasarian classification type II
600
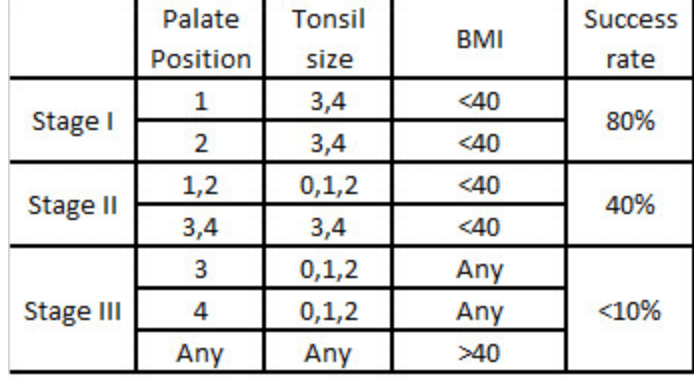
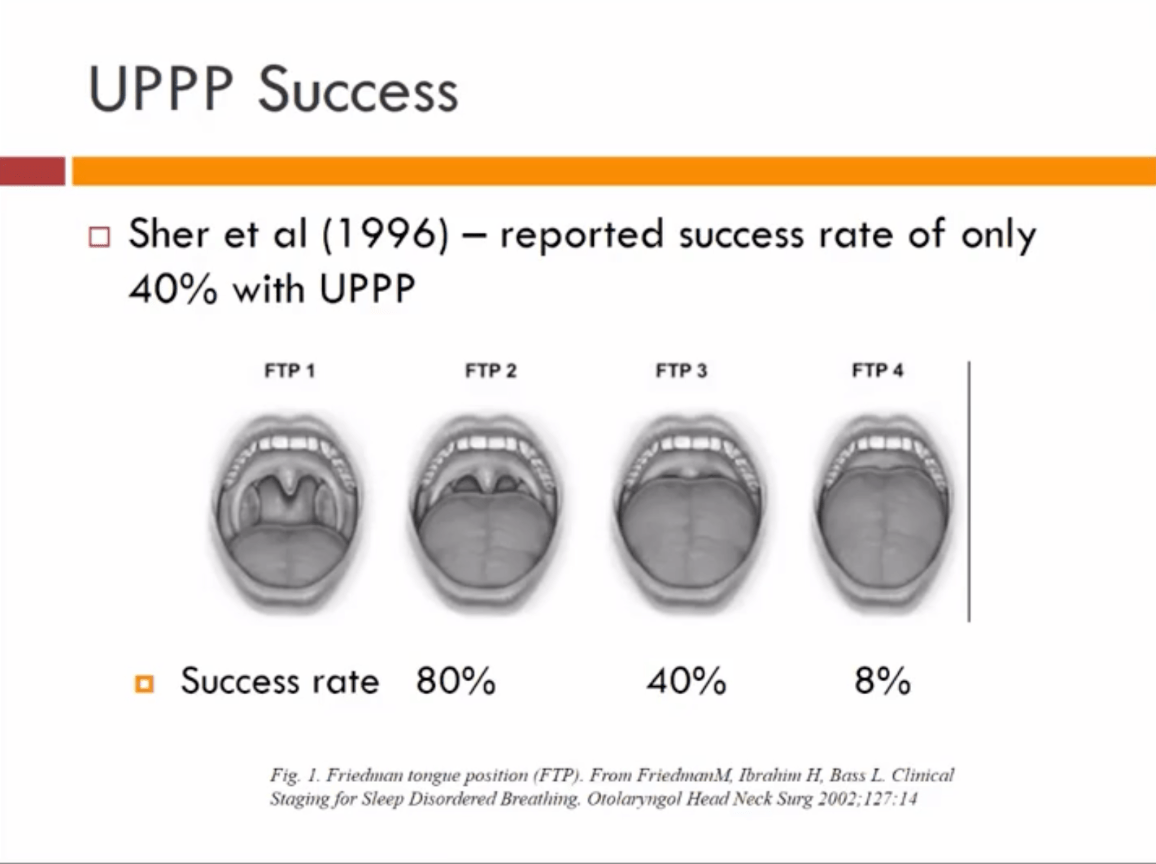
Oral/OP exam shows 3+ tonsils, and a full view of the uvula but not the tonsils without the patient sticking out his tongue. BMI is 39. Chances for success with UPPP?
80%
600
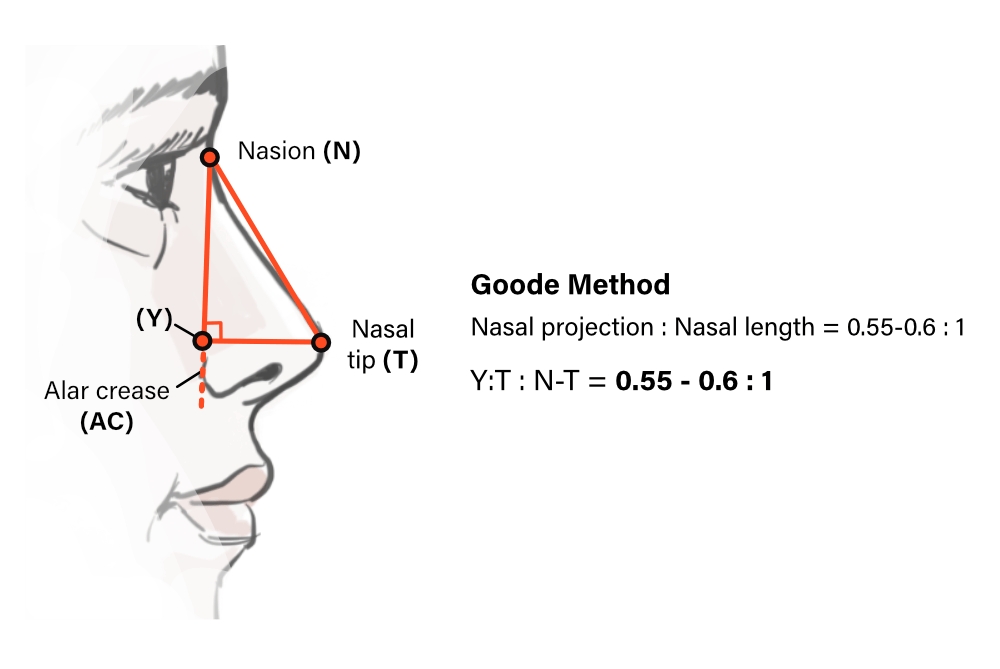
Using the Goode method, this is the ideal ratio of the alar groove–to–nasal tip distance compared with the nasion–to–tip length.
What is 0.55 to 0.60
800
What are the causative species of rhinoscleroma and rhinosporidiosis
800
Issues in what week of cochlear development leads to Mondini malformation?
What is week 7 of development.
- Cochlear development begins week 3. Incomplete partition is the most common malformation of the cochlea. This occurs due to abnormal development of the cochlea during week 7, and results in 1.5 (1-1.5) turns instead of the 2.5 turns in a normal cochlea.
- Week 3: complete labyrinthine aplasia (or Michel deformity)
- Week 4: common cavity to the cochlea &vestibule
- Week 5: cochlear aplasia
- Week 6: cochlear hypoplasia
- Week 7: incomplete partition, dilatational defects, Mondini dysplasia

800
What type of test is performed as a newborn hearing screening for a full term infant (not NICU) and what part of the cochlear does it test?
What is Otoacoustic Emissions (OAE) and Outer Hair Cells?
New Born Screening (OAE/DPOAES)
- OAE require normal hearing & normal middle ear
- Misses Auditory Neuropathy (ABR will detect)
- Very high correlation between the presence of OAE and normal hearing sensitivity (96-100% of normal ears demonstrate OAEs)
- TRANSIENT OAE (TEOAEs) (30db still can miss mild hearing loss)
- DISTORTION PRODUCT OTOACOUSTIC EMISSIONS (DPOAES) (55 & 65db signal-- can still have mild-moderate hearing loss & be normal-- easier to obtain/faster)
- PRETERM/NICU: ABR
- ABR if can sleep naturally (or can sedate them in OR)
800
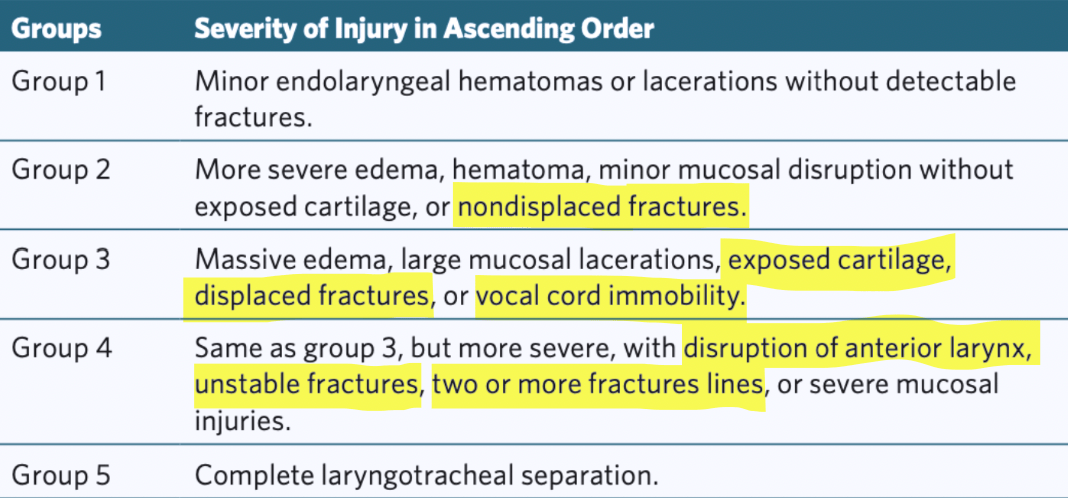
What is the Schaeffer Grade for a patient with a stable displaced thyroid cardilage fracture but with ipsilateral vocal cord cord immobility?
What is Grade 3?
800
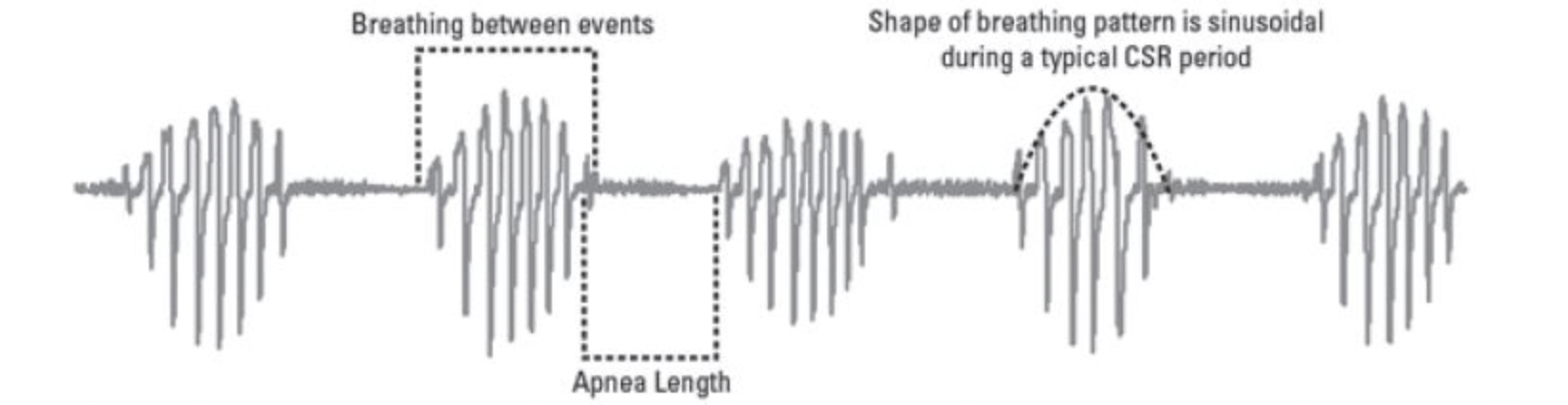
Cheyne-Stokes Breathing criteria
Three cycles of crescendo-decrescendo breathing.
Lasting 10 minutes
ORAssociated with 5 or more central apneas/hypopneas
Associated with heart failure
800
This is the percentage of length lost when rotating a pivotal flap through 180 degrees
40%
- As the degree of pivot increases, the effective length of the flap decreases
1000
You are treating a free flap patient with venous congestion using Hirudo medicinalis, a medicinal leech. You of course know you must prophylactically cover for Aeromonas hydrophilia, which may cause severe NSTI. List four antibiotic options you have for covering this species.
•Fluoroquinolones (Ciprofloxacin, Levofloxacin)Preferred
•3rd gen cephalosporins (ceftriaxone, ceftazidime, cefpodoxime)Preferred
•4th generation cephalosporins (cefepime)Preferred
•Aminoglycosides, preferred if you want to give the patient hearing loss
•Traditionally acceptable but now with resistance: Sulfa (Bactrim), tetracyclines (no credit for these)
1000
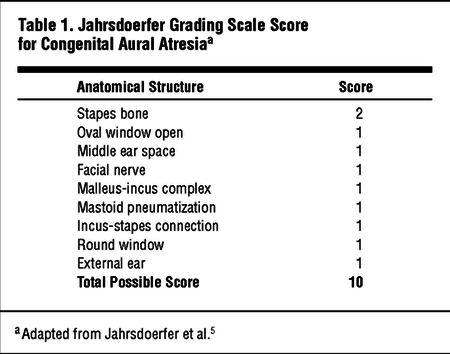
What is the Jahrsdoerfer score for an aural atresia patient with a tympanic membrane, middle ear, malleus, incus, stapes, oval window, round window. No mastoid or facial nerve. Grade IV microtia.
What is 7 points?
Scores 6 through 10 range from marginal to excellent candidates for surgery, whereas a score of five or less usually points to a poor outcome.
1000
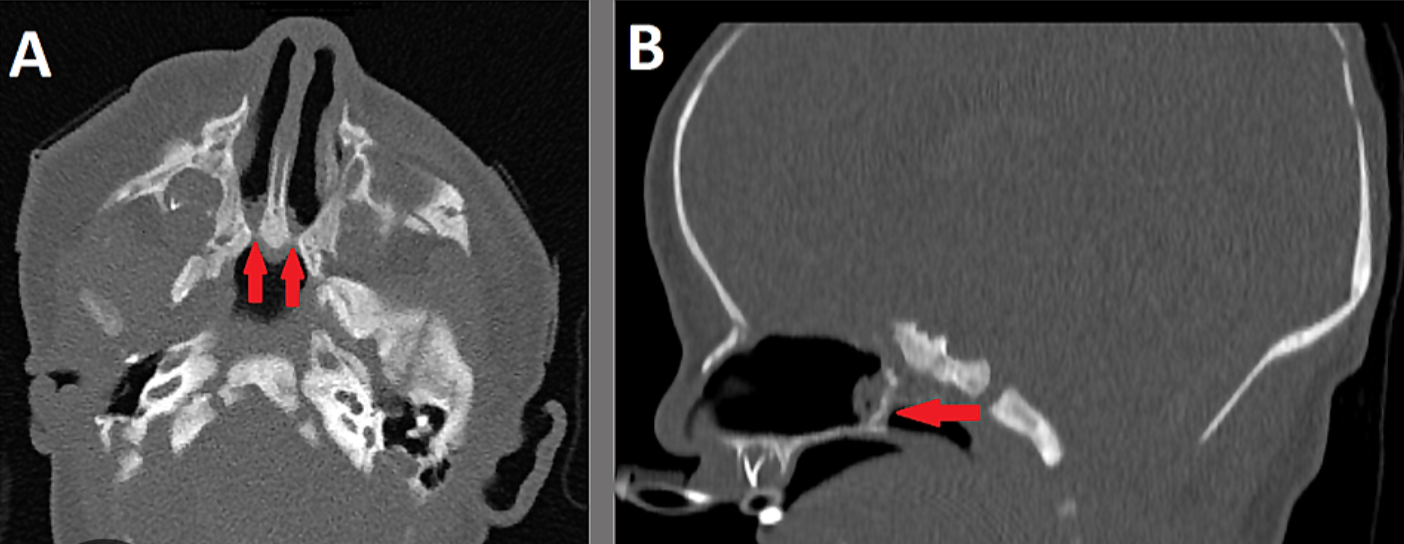
A neonate w cycles of apneas of cyanosis followed by crying, found to be unable to pass 6fr catheter through bilateral nose, what is diagnosis (based on this prompt) & name 2 syndromes associated with it?
What is Bilateral Choanal Atresia?
- a/w CHARGE, Treacher Collin's (AD 1st/2nd branchial arch mal), Crouzon, Apert, Trisomy 21, DiGeorge (22q11 deletion)
- 50% unilateral, 75% bilateral cases a/w syndrome
- CHARGE (MC): Coloboma, Heart Defects, Choanal Atresia, Retardation, hypoGonadism, Ear abnromalities--Get ECHO
- Repair: Bilateral--first few weeks of life, Unilateral: ~6-12 months
1000
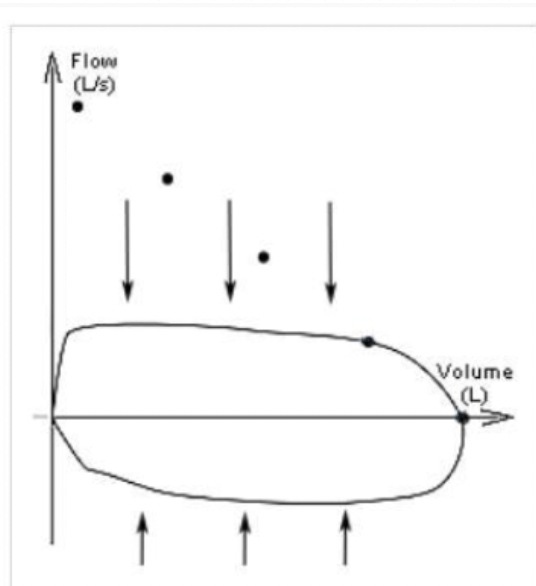
What common pathology is associated with this flow volume loop?
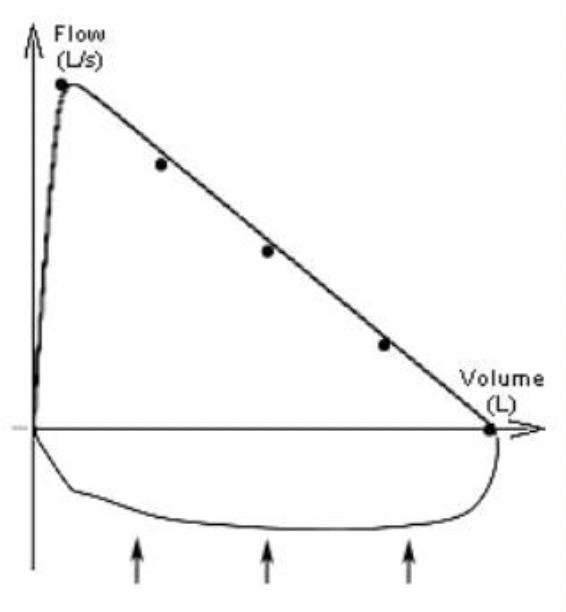
What is vocal cord paralysis? (variable extrathoracic obstruction)
In vocal cord paralysis, the inspiratory curve will be flattened due to narrowing and increased resistance at the level of the glottis. However, expiration will force the vocal cords apart and thus the expiratory curve will be normal or near normal.
- Fixed extrathoracic lesion
1000
Lateral Cephalometric Study Predisposing Factors for OSA (5/6)
Cephalometric Factors Associated with Higher OSA Risk
Posteriorly positioned mandible
Reduced Posterior Airway Space (PAS) (<10 mm)
→ Narrow retrolingual airwayElongated soft palate (>40 mm)
→ Increased velopharyngeal obstruction riskIncreased MP–H distance (>15–20 mm)
→ Inferiorly positioned hyoid / tongue baseIncreased lower facial height / steep mandibular plane angle
→ Vertical growth pattern, airway instabilityMacroglossia (relative tongue size > oral cavity volume)
1000
This rhinoplasty complication occurs with aggressive dorsum resection without osteotomy
Open roof: aggressive dorsum resection without osteotomy à gap between dorsal septum and lateral nasal wall
Vs inverted V: disruption of keystone area à cartilaginous septum sinks in creating inverted V and mid vault collapse

