Liver
Gallbladder
Pancreas
Spleen
Miscellaneous
100
3yoM p/w nausea/vomiting x1 after being found on the floor with an open bottle of acetaminophen 4 hours prior. Serum acetaminophen level is above the Rumack-Matthew Nomogram. What is your next step? (Extra 200 points if you can correctly specify PO or IV dosing)
N-Acetylcysteine.
PO Dosing: 140mg/kg loading dose, followed by 70mg/kg PO q4h x17doses
IV Dosing: 150mg/kg loading dose, followed by 50mg/kg over 4hr, then 100mg/kg over 16hr
NAC MOA: NAC restores glutathione so that
toxic NAPQI + glutathione -> nontoxic conjugates
100
What makes up Reynold's Pentad?
1. RUQ abd pain
2. fever
3. jaundice
4. hypotension
5. AMS
100
40yoM w EtOH use and biliary colic, p/w vomiting, and epigastric abd pain radiating to the back x12h. LFTs slightly elevated, lipase >1000. What is this patient's management (include any dietary restrictions)?
Pancreatitis Management:
-aggressive fluid management - to prevent hypovolemia and maintain organ perfusion
-pain management
-PO as tolerated
*no abx!*
100
A 17yoM presents w 1wk of severe sore throat, fever, & fatigue. A rapid strep test is negative. Exam shows posterior cervical lymphadenopathy and marked splenomegaly. What is the likely diagnosis?
Infectious mononucleosis.
100
If pts have a severe PCN allergy, what antibiotic should be used to prevent infectious complications in a pt w variceal hemorrhage?
Ciprofloxacin.
200
51yoM p/w vomiting. LFTs wnl. CTAP shows diffuse heaptosteatosis. Sx improve, pt is stable for discharge. What is the next step/disposition?
Discharge w outpatient primary care f/up and recommend abstinence from alcohol.
Metabolic Associated Steatosis Liver Dz:
Risk factors - obesity, HTN, DM
sx - typically asymptomatic, but can present w n/v, RUQ abd pain.
on exam - nontender hepatomegaly, mild/moderate elevated AST/ALT
200
Name 4 findings found on Bedside POCUS that suggest acute cholecystitis.
1. cholelithiasis
2. sonographic Murphy's sign
3. thickened gallbladder wall >3mm
4. pericholecystic fluid
200
Physical exam findings concerning for necrotizing pancreatitis?
Grey-Turner sign: flank ecchymosis
Cullen sign: umbilical ecchymosis
Both signs suggest retroperitoneal bleeding 2/2 pancreatic necrosis.

200
Asplenic patients presenting with fever are at increased risk for developing sepsis; in regards to medical management, you need to collect blood cultures and give antibiotics targeting what organism?
S. Pneumoniae.
abx: Ceftriaxone +/- Vancomycin
200
What condition does a patient with jaundice after fasting and isolated unconjugated hyperbilirubinemia have?
Gilbert Syndrome.
Mutation in UGT1A1 gene -> decreased enzyme activity that converts unconjugated bilirubin to conjugated bilirubin
presents w intermittent jaundice.
triggers: fasting, intercurrent febrile illness, physical exertion, stress, menses
300
A 35yo injection drug user presents w RUQ pain, vomiting, and jaundice. A viral hepatitis panel returns w HBsAg+, anti-HBc IgM+, and HBeAg+. What is the most likely diagnosis?
Acute Hepatitis B infection.
HBsAg+ -> indicates Hep B virus is present
anti-HBc IgM+ -> recent HBV infectionHBeAg+ -> indicates high viral load
300
44yoF w obesity, HTN, HLD p/w RUQ abd pain after eating lunch, radiating to R shoulder. HR 120bpm. Exam notable for scleral icterus and epigastric tenderness. What imaging study is the most sensitive noninvasive diagnostic modality for her condition?
MRCP.
MRCP has 93-94% sensitivity and specificity to detect common biliary duct stones.
*transabd US is more sensitive for gallstones, but not for CBD stones.
*ERCP is invasive - but is both diagnostic and therapeutic!
300
Name the complications of acute pancreatitis.
-Pancreatic pseudocysts
-Pancreatic necrosis
-pancreatic pseudoaneurysm
-ARDS
300
A 4yoM w family history of sickle cell disease, presents 3days into a viral illness course with abdominal pain, pallor, splenomegaly, and soft blood pressures. Labs are notable for elevated reticulocyte count, palpable splenomegaly, and very low hemoglobin. What complication of sickle cell disease is happening?
Splenic Sequestration Crisis.
path: rapid sequestration of RBCs in spleen causing splenomegaly and severe anemia, often occurring in children 6mo-6yrs old in the setting of a viral illness.
management:
-hemodynamic support
-pRBC transfusions PRN
-splenectomy for recurrent events
300
A well-appearing woman is incidentally found to have small calcifications about the gallbladder on an abdominal plain film; a diagnosis of "porcelain gallbladder" is subsequently confirmed on abdominal CT. What is the best next step in management?
A. obtain emergent surgical consultation for cholecystectomy d/t risk of perforation
B. admit for ERCP to remove suspected calcified stones
C. Refer for palliative tx of advance cholangiocarcinoma
D. Advise her of the increased risk of gallbladder cancer and refer for elective cholecystectomy
D. Advise her of the increased risk of gallbladder cancer and refer for elective cholecystectomy.
-Porcelain gallbladder has little risk of acute obstruction or perforation.
-3% of pts w porcelain gallbladder will develop cancer of the gallbladder.
400
21yoM w fever/chills, RUQ abd pain, nausea after returning from international trip from Mexico 1mo prior. Abd US shows liver mass w well-circumscribed borders and a hypoechoice center. What is the recommended management for this patient?
Oral microbials.
Entamoeba Histolytica
sx - fever/chills, n/v, RUQ pain, diarrhea. +/- wt loss, malaise, anorexia. jaundice is rare.
dx - single hypoechoic lesion on right upper lobe of liver on imaging
tx - metronidazole + paromycin*
*intraluminal - otherwise, risk reinfection from cysts w/in gut!
400
72yoM w wt loss over the past month w abd pain, white-colored stool, jaundice. CTAP shows a mass concerning for cholangiocarcinoma. What is the strongest risk factor in the US for this diagnosis? (Bonus 400points if you can name the strongest risk factor in China, Korea, and eastern Russia.)
In the US: Primary Sclerosing Cholangitis.
PSC pts carry a 5-10% lifetime risk of developing cholangiocarcinoma.
In China/Korea/eastern Russia: trematode Clonorchis Sirensis (aka Chinese liver fluke).
Contracted by eating raw/undercooked fish. Tx: Praziquantel
400
A 60yoM presents with several weeks of very mild, dull aching abdominal pain, decreased appetite, and fatigue. Today, family noticed a yellow discoloration to his eyes. What is the likely diagnosis?
pancreatic cancer.
The classic presentation of pancreatic cancer is painless, progressive jaundice.
400
34yoF w SLE on therapy, p/w epigastric and LUQ abd pain w splenomegaly on exam. Refer to following picture; what is this patient's diagnosis?
Portal vein thrombosis.
management depends on whether pt is a cirrhotic or not: possible anticoagulation for cirrhotics.
400
What is the criteria you use to predict mortality and determine the need for a liver transplant in a patient with acute liver failure?
King's College Criteria.
types: Acetaminophen vs non-acetaminophen associated liver failure
factors: pH, coags, age, hepatic encephalopathy grade, bilirubin
500
57yoF w abd pain, n/v, jaundice x3d. Which of the following lab values is most suggestive of acute hepatitis A as the cause of this patient's sx?
A. AST 100, ALT 120, Tbili 6.5
B. AST 250, ALT 100, Tbili 2.5
C. AST 40, ALT 55, Tbili 1.5
D. AST 6000, ALT 6500, Tbili 3.0
E. AST 950, ALT 1100, Tbili 4.0
E - AST 950, ALT 1100, Tbili 4.0
Acute viral hepatitis: AST & ALT range 300 - 3000
500
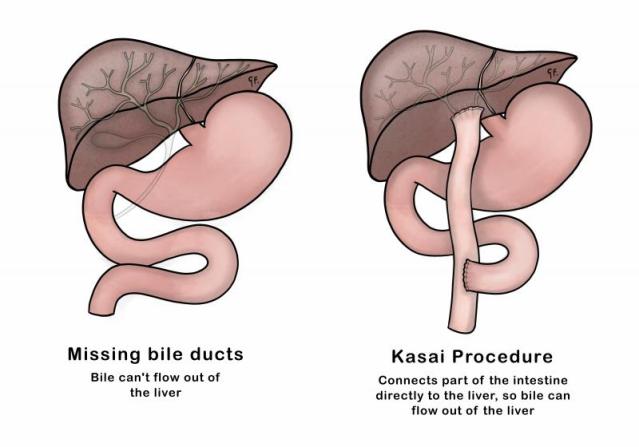
Name a congenital pediatric condition that can present with acholic (clay-colored) stools.
(Bonus 200pts: you can name the appropriate intervention/medical management for this condition and what it entails)
Biliary Atresia
path: inflammatory destruction of bile ducts
sx: usually peri/postnatal.
-prolonged neonatal jaundice (outside 1st week ofl ife)
-conjugated hyperbilirubinemia
-hepatomegaly
-acholic stools, dark urine
management: Kasai surgery (or Liver transplant)
500
A key component of medical management for pancreatitis is volume resuscitation. What clinical targets do you use to ensure that you achieve adequate volume resuscitation? (3 major targets)
1. HR <120bpm
2. MAP 65-85
3. UOP 0.5-1mL/kg/hr
500
Name 2 out of the 5 tropical diseases that can lead to splenomegaly.
Tropical Diseases:
-Malaria
-Trypanosomiasis
-Typhoid
-Brucellosis
-Schistosomiasis
500
What is the best way to increase kidney perfusion in a pt w liver cirrhosis in whom hepatorenal syndrome is suspected?
splanchnic vasoconstriction with vasopressors.
Hepatorenal Syndrome
Path: portal hypertension/congestion -> dec systemic vascular resistance -> activate RAAS
triggers: GI bleed, bacterial infx
tx: MOA therapy
Midodrine - alpha1 agonist
Octreotide - splanchnic vasoconstriction
Albumin - intravascular volume expansion