Inflammation Nation
Just Not My Type
Joint Drama 101
ANA You Glad you Tested?
It's Not That Complicated
200
Define Arthritis in JIA
The presence of joint effusion or any 2 of the following: increased warmth, limitation of range of motion or pain with range of motion
The arthritis must be present At least 6 weeks beginning before the 16th birthday
200
What is undifferentiated JIA?
A patient presented with arthritis that does not clearly fit with 1 of the other subtypes or with features of more than 1 JIA subtype
200
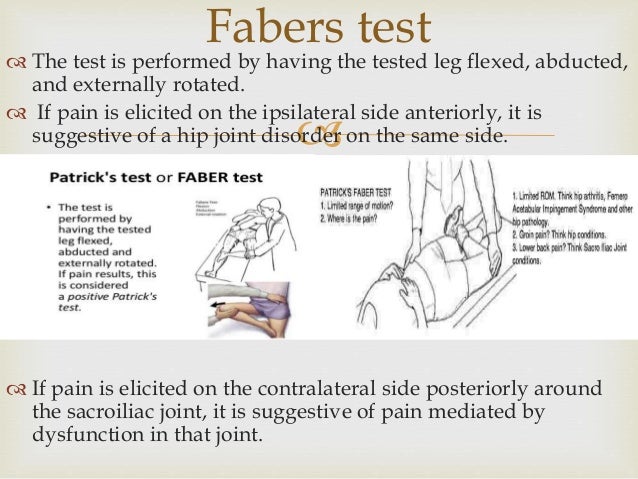
What is the FABER test and what is a positive test?
FABER (Flexion, ABduction and External Rotation) test - the hip is actively abducted in flexion and external rotation.
A positive test elicits pain in the sacroiliac region
200
Initial monotherapy in treatment of oligoarticular disease or systemic onset JIA?
NSAIDs
Also used as adjunctive therapy in other patients. If children experience GI adverse effects from nonselective NSAIDs, they may benefits from selective cyclooxygenase-2 inhibitors such as celecoxib.
200
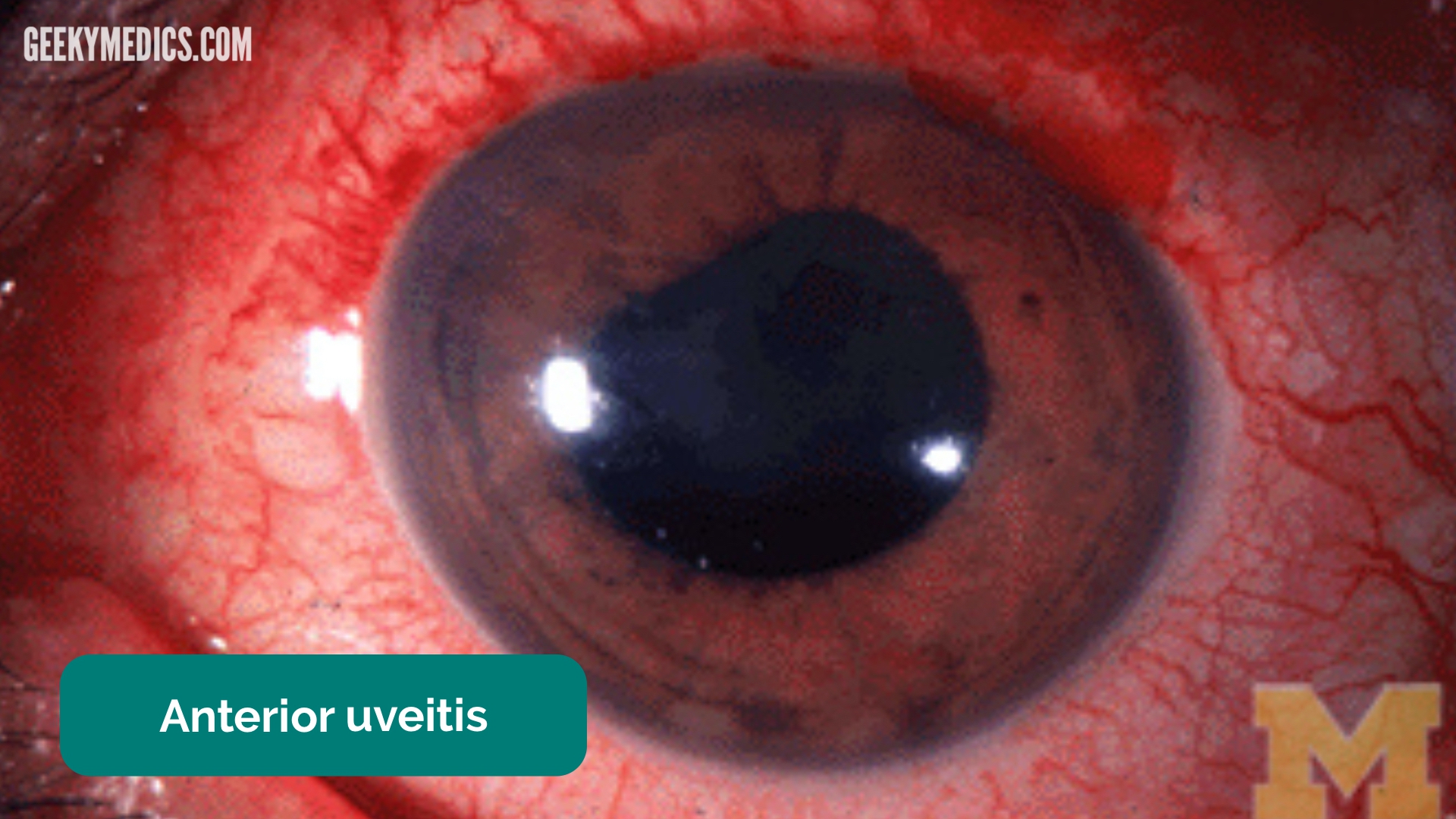
Two highest risk groups for Uveitis
Young children with oligoarticular JIA and ANA positive
Polyarticular JIA and ANA positive
Ophthalmologic screening with slit lamp examination at regular intervals is essential to detect asymptomatic uveitis.
400
Inflamed and hypertrophied arthritic synovium also known as
Pannus
400
Oligoarticular JIA affects no more than ___ joints within the first ____ months of disease onset.
Oligoarticular JIA affects no more than 4 joints within the first 6 months of disease onset.
It is the most common subtype and accounts for approximately 50% of all cases. Peak incidence is between 2 and 4 years of age.
400
These joints are involved in Oligoarticular JIA
Knee is the most frequently involved joint.
Isolated hip involvement is rare
400
Besides rheumatoid factor, RF positive Polyarticular JIA also show positivity for this antibody.
Anti-citrullinated peptide antibody
400
Temporomandicular joint arthritis should be screened by which modality of choice?
Magnetic Resonance Imaging (MRI)
600
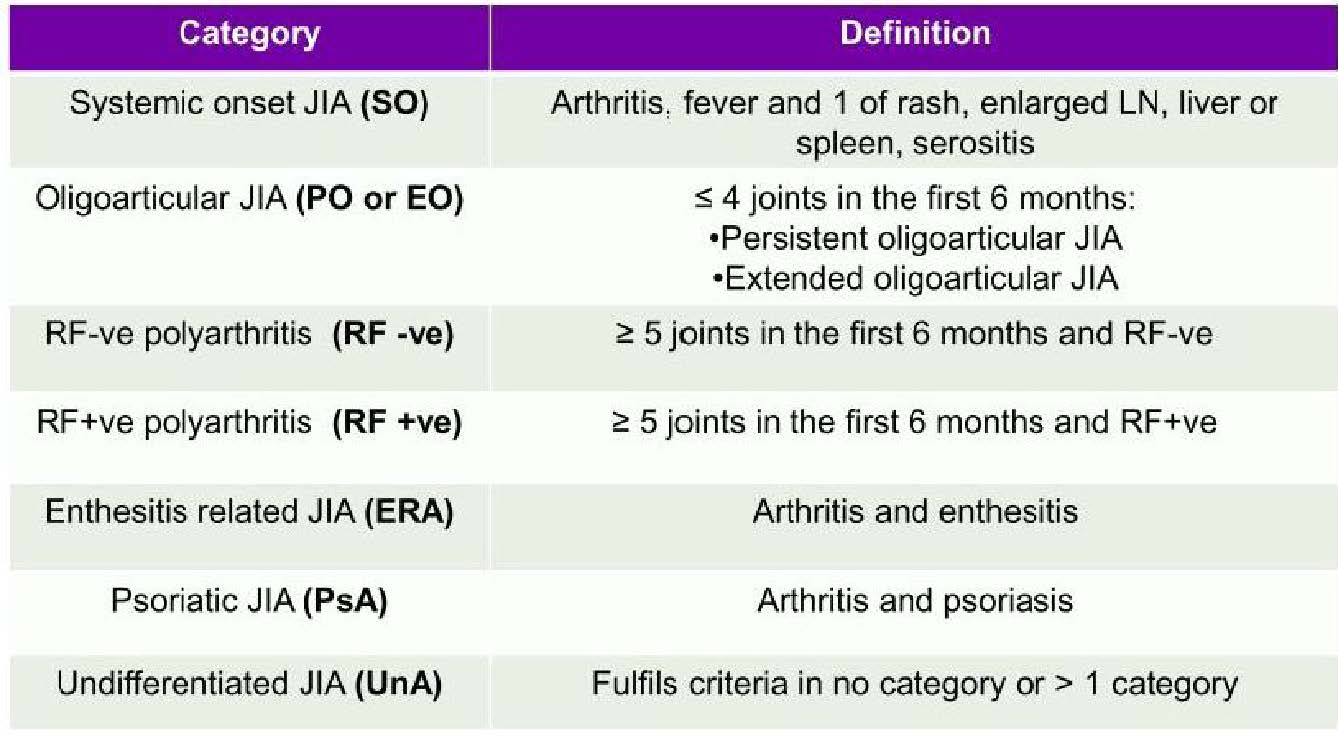
Name the 7 subtypes of JIA
What is Oligoarticular, Rheumatoid factor (RF)-negative polyarticular, RF-positive poly articular, systemic-onset JIA, enthesitis-related, juvenile psoriatic and undifferentiated arthritis?
600
Polyarticular JIA affects ___________ during the first 6 months of disease.
Polyarticular JIA affects 5 or more joints during the first 6 months of disease
It is further subdivided based on serological status as the presence or absence of RF
600
Enthesitis-related Arthritis demonstrates inflammation where?
At the insertion sites of tendons and ligaments into bone in addition to arthritis.
It is more common in boys and has a mean age of onset in middle to late childhood. Children often present with asymmetrical, lower extremity-predominant arthritis and frequently have concomitant tenderness at sites such as the Achilles tendon and plantar fascia insertions.
600
Name 5 of 8 expected laboratory studies for Systemic-onset JIA
Elevated ESR, Elevated CRP, Elevated ferritin, thrombocytosis, normocytic anemia, elevated transaminases, leukocytosis and negative ANA.
600
Prolonged use of glucocorticoids to treat JIA leads to:
Growth failure and osteoporosis
800
We both have bimodal peaks and affect females more than males
RF-negative Polyarticular JIA and Juvenile Psoriatic Arthritis
RF-negative Polyarticular JIA peaks in early childhood (2-4 years) and later childhood/early adolescence ( 6-12 years)
Juvenile Psoriatic Arthritis peaks in early childhood (2-4 years) and 9-11 years
800
This child can be diagnosed with Juvenile Psoriatic Arthritis if 2 of what are present:
Skin psoriasis in a first-degree relative, nail pitting and dactylitis (fusiform swelling of an entire digit that extends beyond the joint margins)
800
This subtype resembles adult-onset zero positive rheumatoid arthritis and has a predilection for small joints of hands and feet.
RF-positive polyarticular JIA resembles adult-onset seropositive rheumatoid arthritis typically presenting with symmetrical polyarthritis with predilection for the small joints of hands and feet.
Incidence is highest in teenage girls.
800
Methotrexate is the initial DMARD of choice for management of _______ and _______ JIA. Regular lab monitoring for _______ or _______ is recommended.
Methotrexate is the initial DMARD of choice for management of severe oligoarticular and polyarticular JIA. Regular lab monitoring for cytopenias or elevated transaminases is recommended.
800
Macrophage Activation Syndrome and interstitial lung disease is associated with which subtype?
Systemic-Onset JIA
1000
Diagnosis of Systemic-onset JIA requires:
The presence of daily fever for 2 weeks (quotidian pattern, > 39C/102.2 F followed by rapid return to normothermia) and a characteristic evanescence salmon-colored polymorphic rash, typically evident during episodes of fever. The rash is non-prurience and predominantly affects the trunk and proximal extremities. Arthritis presents 1 to 3 weeks after fever onset.
1000
I‘m part of the family with inflammatory bowel disease and ankylosing spondylitis. What am I called and what else am I associated with?
Enthesitis-Related JIA has a strong association with Human Leukocyte Antigen (HLA) B27
1000
This happens at the level of joint tissue in JIA pathogenesis
Synovium thickens in early JIA, with proliferation of synoviocytes and infiltration of T cells, B cells, natural killer cells, macrophages, dendritic cells and neutrophils. Synovial proliferation causes intra-articular hypoxia with enumeration of proangiogenic factors including vascular endothelial growth factor and angiopoetin-1.
1000
Name 3 Tumor necrosis factor alpha inhibitors
Etanercept, Adalimumab and Golimumab
1000
Name the complication associated with oligoarticular JIA
Leg length discrepancy if inadequately treated. The affected leg experiences an initial period of accelerated growth caused by the presence of increased blood flow and growth factors in the inflamed joint, but the leg will eventually be shorter than the unaffected limb as the patient approaches skeletal maturity and the growth plate closes prematurely.