Blood gone wild
Breathless and confused
Heart drama
Pee and Poo
Pharmacy strikes back!
100
33 y/o vegetarian queen comes w/weakness, fatigue, and cravings of eating ice chips all the time! the smear shows:

What does this patient have??
IRON DEFICIENCY ANEMIA!
Loss or poor intake/absorption (Dont forget the ppis)
low ferritin (always first to go), low iron, high TIBC.
tx > oral iron first! best practice << every other day to increase absorption, add vitamin C.
Expect hb increase in 2-3 weeks!!! and should c/w tx 3 months after hb is normal!
-dont treat w/o first looking for a cause, we could miss GI malignancy
-dont stop iron too early
-giving BID/TID iron (worse absorption)
100
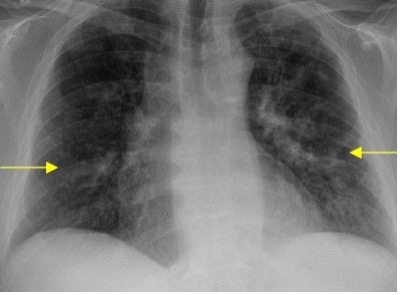
77 yo M found down brought to the ER, noted to have ck 10K, srum creat 6, K 8, hco3 10, nephrology recommending HD, you do your first dialysis catheter and is all good but then you get called that the patient is tachycardic, tachypneic, hypoxic and the xray showes you this
 What to do next ???
What to do next ???
call ct surgery, IR or Dr. Maci, this patient needs a chest tube for pneumothorax!!!
100
64 y/o M was enjoying his steak and got into an arguments with his neighbor, suddently he develops chest pain.
In the ER EKG showed ST elevations in II-III-aVF.
Which coronary artery is most likely occluded ????
RIGHT coronary artery!
$50 bonus >> the patient develops hypotension after nitro, next step ??
100
Your neighbor finds out you are a doctor and is now asking for medical advice, he has history of calcium oxalate stones and states he is drinking a looot of water but he is still passing them. He wants to know if there is any changes in his diet he could do to decrease the risk of calcium oxalate stone formation.
Besides increase water intake what other advice you have for your neighbor?
DIETARY interventions for calcium oxalate stones:
LOW salt intake >> will decrease calcium renal reabsorption. DO NOT TELL PEOPLE TO DECREASE CALCIUM INTAKE, this will decrease oxalate absorption in the GI tract.
low protein diet >> will decrease urinary calcium excretion, low oxalate diet (spinach)
Increase in potassium and citrate!! good for the stones and the heart
2L water per day!
100
68 y/o M with afib on warfarin admitted for pna, started on azithromycin. INR increases from 2.3 >>5.8
what is the mechanism behind this interaction?
Inhibition of warfarin meatabolism via CYP450 >> Increased AC effect
BONUS $100 >> Which macrolide is safest with warfarin??????
200
20 y/o F presents to the ER with chest pain, sob and fever! the smear is looking like this:
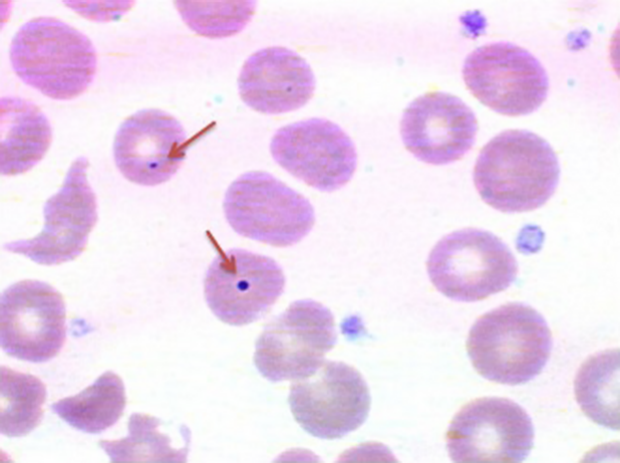
What is the pointed cell? and where do we usually see this??
howell jolly bodies*****
DNA remnants usually removed by the spleen, if seen >> the spleen is not working!
splenectomy, sickle cell, liver disease and rarely in celiac disease.
Encapsulated bugs >>pneumo, meningo, h influenzae, fever and this smear >> ceftriaxone!
200
68 y/o M with COPD c/w worsening sob, ABG shows:
ph 7.28, CO2 68 HCO3 31. You start high flow but o2 hour later his mental status worsens... what is the most likely mechanism of this deterioration?
a. loss of hypoxic respiratory drive
b. increased dead space ventilation
c. worsening V/Q mismatch due to reversal of hypoxic pulmonary vasoconstriction
d. oxygen induced metabolic alkalosis
WORSENING V/Q MISMATCH DUE TO REVERSAL OF HYPOXIC PULMONARY VASOCONSTRICTION.
in COPD we have good and bad alveoli, the body is smart and redirects blood away from bad alveoli, this is called hypoxic pulmonary vasoconstriction. if we turn that off by giving o2 the o2 will go to the bad alveoli causing worsening co2
"hypoxic drive" is NOT the main issue
200
72 y/o M passes out at the movie theater while in line for the devil wears prada.
He tells you he felt warmth and w/ nausea and started sweating before the syncopal episode. His wife saw his arms jerking but there was no tongue biting or urinary incontinence. In the ER work up including head CT, EKG, lab work, vital signs, telemety are normal.
what is the next best next step?
a. admit for 48 telemetry monitoring
b. reassure and ask to follow up with pcp
c. 48 h ambulatory EKG monitoring
d. EEG
e. tilt table testing
GO HOME!!
syncope history very important!! in his case he had autonomic prodrome sx consistent with neurocardiogenic (vasovagal) syncope w/o concerning signs.
*framingham heart study >> cardiogenic syncope had no increase in all cause mortality, mi, or cva.
200
First year IM resident signs up for a marathon for the first time! as soon as he is done he is all sweaty and tired and then he starts to have nausea, vomiting and is brought to trident. In the ER he is having seizures!!!!

If you had to guess, how is his urine osmolarity going to be and why?
HIGH!!!
this person is loosing salt and water with sweat, the body will try to conserve water by turning on ADH, causing water retention AND this person is drinking hypotonic fluids making things worst.
200
hospitalized patient on vanc and ceftriaxone develops flushing and redness to the face and upper chest during infusion
what is this reaction called????
RED MAN SYNDROME
WHY?
-direct mast cell degranultion
histamine release
vasodilation
looks like allergy but its not!
tell the nurse to run it slowly
300
You get a call from 3rd floor nurse about a patient who she just started minutes ago a blood transfusion, the patient is having fever, chills, flank pain and dark urine! She is asking if she should stop the blood.
What reaction is this patient having?
Acute hemolytic transfusion reaction!!
ABO incompatibility, rareeeee, presentation in minutes. Stop Blood!
others >> febrile non hemolytic, does not happen right away and is only fever. ok to c/w blood w tylenol >> very common
allergics > urticaria and anaphylactic (angioedema)
TRALI >> ARDS like >> supportive
TACO >> volume overload >> diuretics
300
29 y/o M presents to the ER with sudden sob, headache and bluish discoloration of his lips right after a party where he admits he inhaled some drugs. he looks cyanotic lungs are clear, his o2 is 82% and does not change with supplemental O2.

his blood looks dark, ph 7.41, co2 39 and o2 is 102.
What is the most likely diagnosis??
methemoglobinemia!!!!
hemoglobin iron gets oxidized and it cant carry o2 and the remaining normal hb holds onto o2 tighter! so tissues gets less oxygen! so patients are blue looking from cyanosis, the blood looks dark and the puls ox will stay at 85% even with o2.
pulse ox stuck at 85% + normal Pao2 is methemoglobinemia until proven otherwise!!
causes: benzocaine/lidocaine sprays, nitrates (poppers), sulfas. dx >> co-oximetry (abg w/co oximetry, will measure methemoglobin)
tx >> methylene blue!
300
68 y/o M c/f LHC s/p stent, you are working on the DC, cards rec clopidogrel and aspirin. The patient tells you he had history of gastritis in the past. so you plan to send him with gi protector!
WHICH PPI should you AVOID ??????
OMEPRAZOLE!!!
They inhibit CYP2C19 which is required to activate clopidogrel. putting him at risk of thrombosis.
ok to use pantoprazole (minimal CYP2C19 effect)
ppi tx does no affect prasugrel or ticagrelor.
* in high risk patients taking dapt and ppi decreases risk of upper GIB *
300
55 y/o M with PMH alcoholic cirrhosis, presents with hematemesis and hypotension.
You are going to give the MUST GIVE med on this patient with cirrhosis and GIB, what cv side effect you should worry about and in which patients should you be cautions?
BRADYCARDIA!!
octreotide >> somatostatin analog, causes decrease in splanchnic blood flow which is good for varices BUT also decreases HR.. avoid/caution in patient with baseline bradycardia.
$ bonus 50 >> besides octreotide what other medication you should start??
300
55 y/o F admitted for MRSA bacteremia, started on dapto, dificult dispo, on week 3 when we are ready to send her home she started to complain of sob, cough, she had fevers, her labs showed peripheral eosinophilia, she is hypoxic. the xray is showing
What is the most likely dx and next best step??????
Daptomycin eosinophilic pneumonia!!!
usually 2-4 weeks after starting dapto, classic sx: respiratory, pulmonary infiltrates and eosinophilia.
dx: BAL confirming eosinophils > 25%
tx > stop dapto asap and start steroids!
400
Rapid response from 6th rehab floor!! 60 y/o M with pmh ESRD on hd, recent knee surgery 5 days ago now with acute hypoxic respiratory failure and tachycardia!
hr 120s, o2 st 85% non rebreather mask
Labs from a week ago were normal
meds: oxycodone, phoslo, lisinopril and heparin for dvt prophylaxis

What is the mechanism of action of the treatment for this patient??
This patient has HIT!
TX Direct thrombin inhibitor!! Argotroban (in liver failure use bivalirudin but cant be use in renal failure).
HIT > Ab PF4 >> low platelets and high risk of thrombosis!!!
The 4T >> 50% drop in Thrombocytopenia, Timing 5-10 days, Thrombosis present? oTher causes ??
-Dont wait for antibody, if suspected treated
-dont give platelets unless bleeding
400
44 y/o M admitted for necrotizing pancreatitis but hospital course is complicated by acute hypoxic respiratory failure s/p intubation. most recent xray:

Blood cultures and urine cultures are negative but his sputum culture grow candida.
what is the next step ?????
Optimize ARDS management with lung protective ventilation!!
DO not give antifungals, broaden antibiotics or repeat cultures.
candida colonization specially in intubated patients is common, candida pna is soo rare!! and it should happen from hematogenous spread! his bc are negative.
400
72 Y/O M admitted with inferior stemi.
6 hours later he is dizzy and hypotensive, the ekg is bellow

what is the appropriate next step ??????
atropine and call EP or card for transcutaneous pacing.
This is a complete av block, seen with inferior MI.
400
You have two patients with cirrhosis!
Patient A here for worsening ascites, hypotension, weakness, rising creat for 3 days and serum na 127. No improv with IVF, bland urine sediment
Patient B here for SBP, on pressors, day 3 creatinine rises despite IVF, na 127, sediment is showing cast.
If you check urinary sodium in this patients, how will it be and why?
Patient A low sodium <10
Patient B high sodium >40
Patient A has HRS, the splanchnic vasodilation makes the kidney sense there is no volume, causing intense renal vasoconstriction and RAAS activation, so kidney is retaining urinary sodium and water.
patient B has ATN, the kidney are not able to increase sodium reabsorption anymore, the tubules are damaged, that's why we see cast on the sediment.
400
 You get a call from a patient that is freaking out because he has bubbles in his PIV, the tech that is in the room immediately stops the iv.
You get a call from a patient that is freaking out because he has bubbles in his PIV, the tech that is in the room immediately stops the iv.
What is the next step?
Calm the patient down. Bubbles in the venous system are harmless! They go to the right side of the heart and then the lungs. You will need more than 100ml of air to cause trouble! But for this not to happen again please ask the nurse to do a better priming!
NOT the same in arterial line!!! A small amount is dangerous!
500
45 y/o M with pmh obsesity and mechanical valve on warfarin admitted for pna. He admits he has not been taking his meds for months, you resumed his home meds. Day of dc he is not on oxygen, wbc 8, hb 10, INR 4, you then see this on his physical exam

Deficiency of what caused this ?????
PROTEIN C!!
Warfarin inhibits II-VII-IX-X AND protein C and S. but protein C depletes very fast causing a transient hypercoagulable state v>> thrombosis of skin vessels >> necrosis >> mostly in fatty areas.
always try to bridge with heparin in high risk patients, do not use high warfarin doses to start
stop warfarin give vitamin K , start heparin and consider protein C concentrate.
$extra 100 bonus >> warfarin was initially used as???
500
50 y/o m from El salvador c/w of hemoptysis. PMH HIV and TB, reports he finished his directly observe therapy of tb 12 years ago and he is compliant with his hiv meds.

What do you think this patient has and what is the treatment??
Aspergilloma!!
mild >> observe
hemoptysis >> surgical resection
NO antifungals, drugs cant reach fungus ball and it oes not fix th bleeding. aspergilloma is a structural problem, not an infectious problem.
not the same a invasive aspergilloma > heere we do treat with voriconazole.
500
Who invented the first EKG machine ??

Willem Einthoven in 1901
*WILD facts:
weighted 600 pounds
patients had to put limbs in buckets of salt water
it took 5 people to operate it
500
40 y/o F comes with chronic diarrhea for 4 months, she reportd 6-8 watery bowel movements, no weight loss, does get better if she stops eating, she is refusing to leave the ER w/o an answer and the ER calls you for admission. Stool electrolytes showed
Na 40 mEq/L
K 15 mEq/L
Calculate the stool osmotic gap and determine the type of diarrhea
Stool osmotic gap >> 180 mOsm/kg, osmotic diarrhea
290 -2 (stool na + stool K)
osmotic, secretory, inflammatory and fatty!
Osmotic caused by non-absorbed substances in the gut that pull water into the lumen (lactose, sorbitol, artificial sweeteners, mg laxative, celiac disease)
gets better when patient stops eating >> osmotic
500
hospitalized patient with bipolar disorder on lithium comes admitted for pna, started on lisinopril for bp and NSAIDS for pain
2 days later the patient develops confusion, tremors, vomiting
what is the mechanism of action of this toxicity?
REDUCED RENAL CLEARANCE OF LITHIUM
1. lisinopril decreases GFR via efferent arteriole dilation
2. saids decrease prostaglandins and cause afferent arteriole constriction.
lithium ace and NSAIDs perfect storm for lithium toxicity via decrease grr