Zonation
Who is he?
NEJM image challenge
Encephalopathy
Markers +
100
What percentage of the blood in liver sinusoids is arterial?
Approximately 75% of the afferent lobule blood is venous blood that drains from the intestine, with only 25% of the perfusion originating from highly oxygenated arterial blood
100

100
A 77-year-old man with metastatic lung adenocarcinoma presented to the emergency department with a 2-week history of dyspnea. Imaging studies showed a pleural effusion on the right side, previously known liver metastases and perihepatic fluid, and new intrahepatic dilatation of the biliary ducts. A chest tube was placed, and the color of the drained pleural fluid was olive brown. What additional pleural-fluid test is most likely to reveal the diagnosis?

Bacterial gram stain and culture
Bilirubin
Cytology
Fungal stain and culture
Triglycerides
The correct answer is pleural-fluid bilirubin levels. Pleural-fluid studies showed a total bilirubin level of 8.2 mg per deciliter and a direct bilirubin level of 7.5 mg per deciliter. The pleural-fluid triglyceride level was normal, and cultures and cytologic studies were negative. A diagnosis of bilothorax was made. Bilothorax occurs when bile flows into the pleural space. In this case, the mechanism was thought to be diaphragmatic defects caused by hepatic metastases.
100
A patient with compensated cirrhosis is admitted with altered mental status. He was recently treated for a urinary tract infection. Which of the following is most likely contributing to his current symptoms?
A) Hypokalemia
B) Use of lactulose
C) High albumin levels
D) Increased hepatic protein synthesis
E) Beta-blocker therapy
Hypokalemia, a common result of diuretic therapy, and alkalosis promote intracellular shift and renal generation of ammonia, worsening HE. Lactulose helps, not harms.
100
Which enzyme is a typical marker of cholestasis along with serum alkaline phosphatase?
γ-glutamyl transpeptidase
200
Gluconeogenesis is carried out by which hepatocytes?
periportal hepatocytes - since gluconeogenesis is an energy-consuming process.

200
A 48-year-old woman with advanced cirrhosis presented with fatigue, jaundice, and abdominal distention. Laboratory studies showed a hemoglobin level of 5.8 g per deciliter (reference range, 12.0 to 15.5), a lactate dehydrogenase level of 1219 U per liter (reference range, 125 to 220), a low haptoglobin level, and an elevated reticulocyte count. Coombs’ antiglobulin testing was normal. The result of a peripheral-blood smear is shown. What is the diagnosis?
Autoimmune hemolytic anemia
Babesiosis
Hypersplenism
Microangiopathic hemolytic anemia
Spur-cell hemolytic anemia
The correct answer is spur-cell hemolytic anemia. The peripheral-blood smear as shown demonstrated acanthocytes, or spur cells, with irregularly distributed surface projections and lacking central pallor. Spur-cell hemolytic anemia is a type of nonimmune hemolysis that occurs in patients with advanced liver disease due to excess membrane cholesterol in erythrocytes.
200
rapid extension-flexion movements of the head and extremities, best seen when the arms are held in extension with dorsiflexed wrists.
200
A 58-year-old man with a history of alcoholic cirrhosis presents with increasing abdominal distension and mild shortness of breath. Physical examination shows a fluid wave and shifting dullness. Paracentesis yields clear yellow fluid. Labs show:
Serum albumin: 2.8 g/dL
Ascitic fluid albumin: 1.0 g/dL
Total protein in ascitic fluid: 0.9 g/dL
WBC in ascitic fluid: 230/µL (80% lymphocytes)
SAAG: ?
Which of the following is the most likely cause of this patient’s ascites?
A) Peritoneal carcinomatosis
B) Cirrhosis with portal hypertension
C) Tuberculous peritonitis
D) Pancreatic ascites
E) Nephrotic syndrome
SAAG is >1.1, therefore, Cirrhosis with portal hypertension
300
A 38-year-old man presents to the emergency department with nausea, right upper quadrant pain, and confusion after intentionally ingesting a large quantity of acetaminophen tablets. Laboratory tests show elevated liver transaminases, prolonged prothrombin time, and metabolic acidosis. A liver biopsy is performed and reveals extensive necrosis around the central veins of hepatic lobules.
Which of the following best explains the regional susceptibility of this area of the liver to acetaminophen toxicity?
A) Higher expression of albumin mRNA in central hepatocytes
B) Increased oxygen tension near the central vein
C) High expression of cytochrome P450 enzymes in pericentral hepatocytes
D) Dominance of gluconeogenesis over glycolysis in pericentral hepatocytes
E) Enhanced urea cycle activity in zone 3 hepatocytes
Pericentral hepatocytes (zone 3, near the central vein) express CYP2E1 and CYP1A2, key enzymes responsible for converting acetaminophen into the toxic metabolite NAPQI.
This region has lower oxygen tension, and detoxification relies heavily on glutathione, which gets depleted in overdose situations.
Histologically, the centrilobular zone is most vulnerable to hypoxia and drug-induced liver injury, particularly from acetaminophen
300
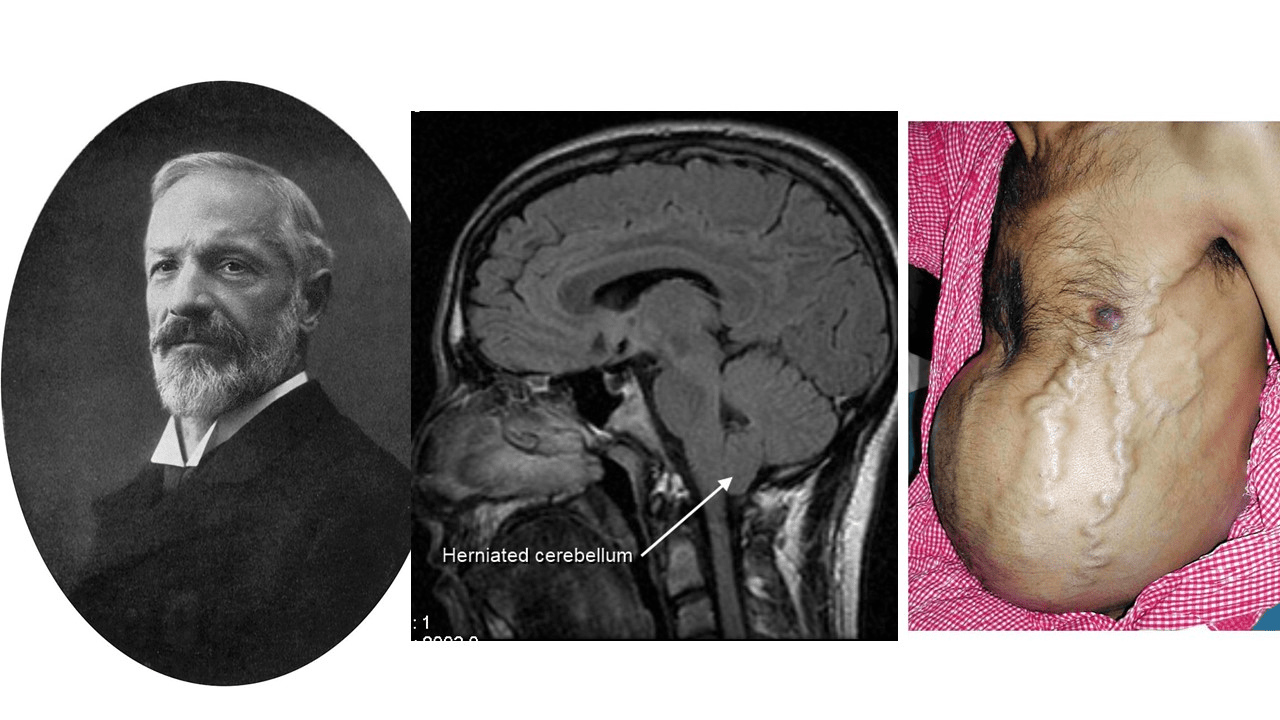
Hans Chiari
300
An 18-year-old man presented with a 2-day history of fever, vomiting, and diarrhea. Three weeks before presentation, he had fallen into a canal. Physical exam was notable for the findings shown in the image. Laboratory studies showed acute kidney injury and elevations in aminotransferase and total bilirubin levels. What is the most likely diagnosis?
Acute hemorrhagic conjunctivitis
Ebola hemorrhagic fever
Giardiasis
Leptospirosis
Subarachnoid hemorrhage
Leptospirosis manifesting as fever, jaundice, renal failure, and hemorrhage was suspected on the basis of the patient’s classic presentation (including the subconjunctival bleeding) and exposure to water with probable contamination by rodent urine. Empirical treatment with intravenous penicillin was initiated. Serum nucleic acid amplification testing identified leptospira species of the serogroup icterohaemorrhagiae. At follow-up 3 weeks later, his symptoms, subconjunctival hemorrhage, and liver and kidney injury had resolved.
300
Why periportal hepatocytes take up glutamine and produce glutamate
Glutaminase activity
Periportal hepatocytes express glutaminase (GLS2), which catalyzes:
Glutamine→Glutamate+NH3This liberates free ammonia (NH₃) from glutamine.
2. Feeding the urea cycle
The released ammonia enters the urea cycle in the same periportal cells, where it's converted to urea:
2 NH3+CO2→UreaUrea is water-soluble and excreted by the kidneys.
3. Oxygen requirement
The urea cycle is energy-intensive, consuming 4 ATP equivalents, so it must occur in well-oxygenated periportal zones.
4. Glutamate fate
The glutamate formed may:
Be transaminated to form α-ketoglutarate (entering TCA cycle)
Be used for glutathione synthesis
Be passed downstream to pericentral hepatocytes, where it's converted back to glutamine by glutamine synthetase (a key scavenger pathway)
300
In which transudative ascites the SAAG < 1.1 ?
Nephrotic syndrome
400
Which zone of the lobule most actively expresses Hamp and Hamp2 genes, which encode hepcidin?
Unlike many other functions, which are mostly active at periportal or pericentral hepatocytes, some are most active at mid-lobule hepatocytes.
400

1878-1937
He described hepatolenticular degeneration in his Gold Medal winning M.D. dissertation of 1912 titled "Progressive lenticular degeneration"
Samuel Alexander Kinnier Wilson
1878 1937
400

A 16-day-old girl who had not yet returned to her birth weight was brought to the emergency department with lethargy. She had tachypnea and marked hepatomegaly with a hepatic bruit, as well as eight small hemangiomas on the scalp, thorax, abdomen, and limbs that had been noted within days after birth. Abdominal ultrasonography showed numerous rounded hypoechoic lesions in the liver (Panel A). Whole-body magnetic resonance imaging showed contrast-enhancing hepatic lesions, as large as 20 mm in diameter, that were hyperintense on T2-weighted images (Panel B)
infantile hepatic hemangiomas
Laboratory studies showed a thyrotropin level of 25.5 mIU per liter (reference range, 0.50 to 8.50) and a reverse triiodothyronine level of greater than 3696 pmol per liter (reference range, 140 to 540). Complications of infantile hepatic hemangiomas include high-output cardiac failure, consumptive hypothyroidism, and bleeding. These vascular lesions typically have rapid growth followed by a phase of slow involution, sometimes over a period of years. Treatment with propranolol, furosemide, and high-dose levothyroxine was initiated. The liver lesions gradually reduced in size, and after 9 months, treatment was stopped successfully.
400
A previously healthy, 38-year-old woman has become increasingly obtunded in the past 4 days. On physical examination, she has scleral icterus, abdominal fluid wave, and asterixis. She is afebrile, and her blood pressure is 110/55 mm Hg. Laboratory findings show a prothrombin time of 38 seconds (INR 3.1), serum ALT of 1854 U/L, AST of 1621 U/L, albumin of 1.8 g/dL, and total protein of 4.8 g/dL. Serum or blood levels of which of the following will most likely be abnormal in this patient?
A Alkaline phosphatase
B Ammonia
C Amylase
D Anti-HCV
E Antinuclear antibody (ANA)
The history points to an acute liver failure from fulminant hepatitis with massive hepatic necrosis. The loss of hepatic function from destruction of 80% to 90% of the liver results in hyperammonemia from the defective hepatocyte urea cycle, and this leads to hepatic encephalopathy within 2 weeks of the onset of jaundice.
400
A patient with ascites has SAAG>1.1.
What additional measurement helps differentiate cirrhosis from right-sided heart failure?
Ascitic protein. Less than 2.5 confirms cirrhosis.
500
Increased alcohol consumption caused an increase in AST levels. What is the likely mechanism?
Pathological conditions that increase hepatocyte oxygen consumption, such as increased alcohol consumption, lead to pericentral hypoxia
500

Hans Popper (1903–1988) – Known as a founding figure of modern hepatology. He extensively studied liver cirrhosis and chronic hepatitis, and co-authored a seminal textbook on liver disease.
500
An 82-year-old man with diabetes presented to the emergency department with fever and confusion. Liver function test showed aspartate aminotransferase level of 1380 u/l (reference range, 5 to 40) and alanine aminotransferase level of 1121 u/l (reference range, 5 to 40). A computed tomographic scan of the abdomen was performed.
What is the most likely diagnosis?
* Acute hepatic necrosis
* Cholecystoduodenal fistula
* Emphysematous hepatitis
* Pyogenic liver abscess
* Ruptured hydatid cyst
Abdominal imaging showed a large area of gas in the right hepatic lobe, suggestive of emphysematous hepatitis. A percutaneous drain was placed, and fluid cultures grew Klebsiella pneumoniae. Emphysematous hepatitis is a rare and fulminant infection of the liver parenchyma that can be seen in patients with diabetes.
500
A 48-year-old man with alcoholic cirrhosis and grade II HE is started on treatment. Which of the following drugs acts by acidifying colonic contents and promoting ammonia excretion?
A) Rifaximin
B) Neomycin
C) Lactulose
D) L-carnitine
E) Metronidazole
Lactulose is a non-absorbable disaccharide fermented by colonic bacteria, producing acidic metabolites that trap NH₃ as NH₄⁺, reducing absorption.
500
A 47-year-old man presents with fatigue and mild jaundice. He takes no medications and denies alcohol use. Physical exam shows scleral icterus but no ascites or asterixis. Labs reveal:
AST: 89 U/L, ALT: 101 U/L, ALP: 410 U/L
Total bilirubin: 3.7 mg/dL Direct bilirubin: 2.9 mg/dLAlbumin: 4.0 g/dL
PT 13 seconds
Which of the following patterns of liver injury is most consistent with these findings?
A) Hepatocellular injury
B) Cholestatic injury
C) Mixed hepatocellular-cholestatic pattern
D) Isolated hyperbilirubinemia
E) Synthetic liver failure
Mixed hepatocellular-cholestatic pattern