ANATOMY
BIOMECHANICS
PATHOLOGY
SPECIAL TESTS
CASES
100
This lumbar vertebra most commonly develops spondylolysis.
L5
Spondylolysis is a stress fracture or defect in the pars interarticularis of a vertebra
L5 experiences the highest mechanical stress in the lumbar spine.
It sits at the lumbosacral junction (L5–S1), where there is:
Significant compressive load from body weight
Repetitive extension and rotation stress (especially in athletes)
This makes the pars interarticularis of L5 particularly vulnerable to stress fractures.
100
Lumbar flexion increases this anatomical space
Intervertebral foramen

100
This condition involves anterior slippage of one vertebra on another.
What is spondylolisthesis?
Bonus question: What are the grades?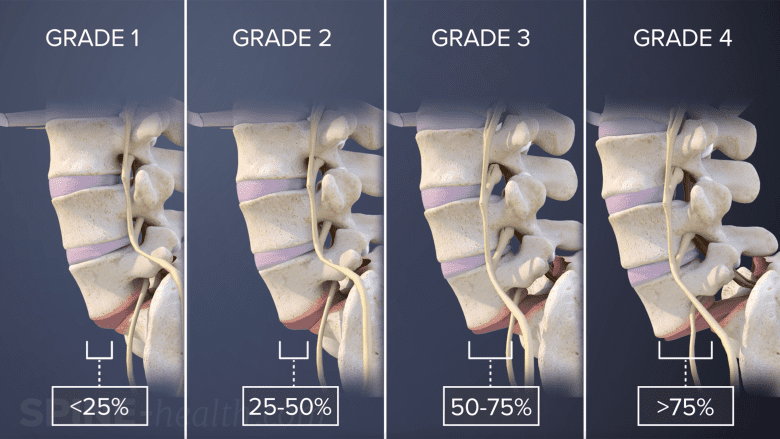
Grade I (0–25%)
Most common. Usually stable.
Activity modification (short term- minimal lumbar extension)
Core stabilization (TA, multifidus, glutes)
Avoid repeated loaded extension early
Grade I (0–25%)
Most common. Usually stable.
Activity modification (short term)
Core stabilization (TA, multifidus, glutes)
Avoid repeated loaded extension early
Gradual return to sport
👉 Majority managed conservatively with excellent outcomes.
Grade II (26–50%)
May be stable or mildly unstable.
Similar rehab as Grade I
Emphasize neutral spine control
Bracing (short term) if symptomatic
Monitor for neuro symptoms
👉 Still primarily conservative, unless progressive neuro deficit.
Grade III (51–75%)
Higher instability risk.
Trial of conservative care if no neuro deficit
Close monitoring for:
Radicular symptoms
Progressive slip
Functional decline
Surgical consult often appropriate
👉 Surgery considered if persistent pain, neurologic signs, or progression.
Grade IV (76–100%)
Significant instability.
Often symptomatic
Higher risk of neurologic compromise
Surgical referral common
👉 Many require surgical stabilization, especially in younger patients.
100
A positive Straight Leg Raise that reproduces leg pain below the knee between 30–70° suggests involvement of this structure.
Lumbar (sciatic) nerve root (radiculopathy)
SLR implicates neural tissue, not just disc.
100
A 40-year-old recreational lifter presents with right buttock pain radiating to the posterior thigh (not past knee). Symptoms worsen with prolonged sitting and repeated lumbar flexion. Extension also produces back pain symptoms. Hip ROM is full, but end-range flexion produces mild buttock discomfort. SLR negative.
What is the primary pain generator?
Most appropriate early exercise strategy?
Discogenic lumbar pain with referral
Core training in neutral position (planks, side planks, bird dogs, palloffs, stir the pot)
*Posterior thigh referral without positive SLR indicates it's not true radiculopathy. but discogenic pain referral (often harder to treat)
200
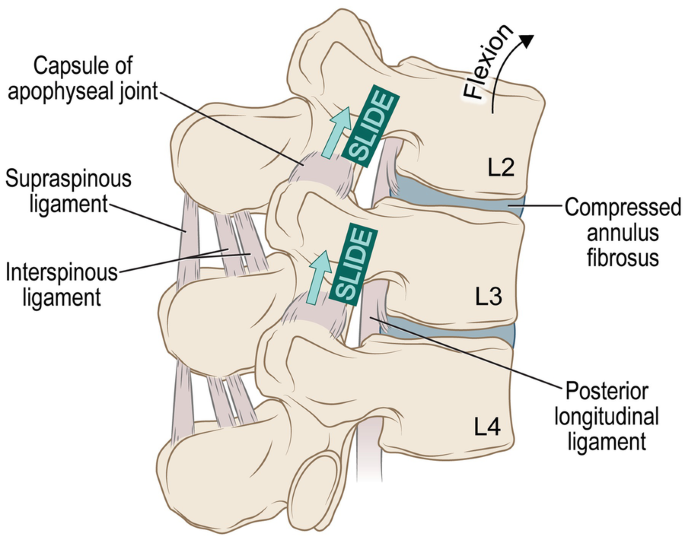
This ligament is the primary passive restraint to lumbar flexion.
Supraspinous ligament or Posterior longitudinal ligament
200
Nutation of the sacrum involves this movement of the sacral base.
What is anterior/inferior movement of the sacral base?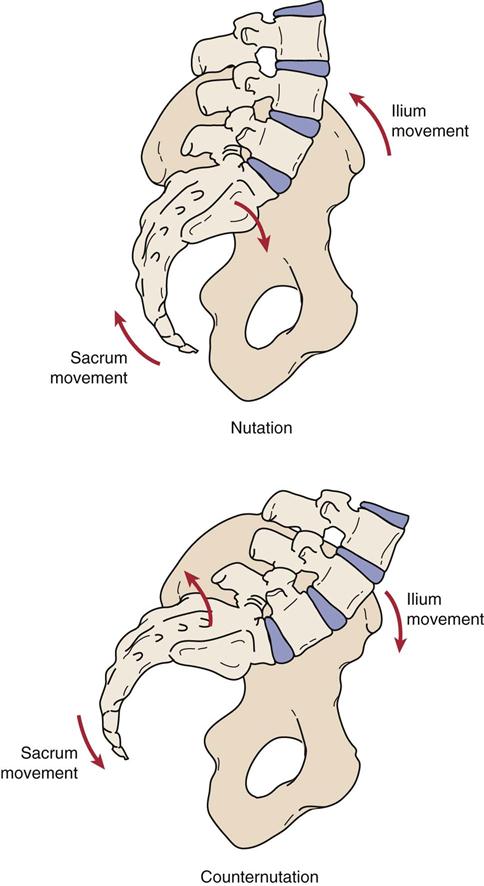
200
This inflammatory condition commonly presents with morning stiffness improving with movement and may involve the SI joints bilaterally.
Bonus question: What is the common blood marker we look for to determine if they have this condition?
What is ankylosing spondylitis?
Bonus answer: HLA-B27
Key points:
Not everyone with HLA-B27 develops disease.
But most patients with ankylosing spondylitis are HLA-B27 positive.
It increases risk - it does not diagnose the condition by itself.
200
These modifications of the Straight Leg Raise increase neural tension and help confirm radicular symptoms.
Ankle dorsiflexion and cervical flexion
200
A 36-year-old postpartum runner reports unilateral lateral buttock pain aggravated by single-leg stance, stairs, and side-lying. Rolling in bed is mildly uncomfortable. Lumbar ROM is full and symptom-free. 2/5 SI provocation tests positive. Resisted hip abduction reproduces pain. Palpation over the greater trochanter is tender.
Primary pain generator?
Most relevant early exercise focus?
Gluteal tendinopathy (greater trochanteric pain syndrome)
Progressive lateral hip loading (isometric → isotonic hip abduction strengthening)
Looks like SIJ. But lateral pain + load intolerance + abduction pain points to tendon.
300
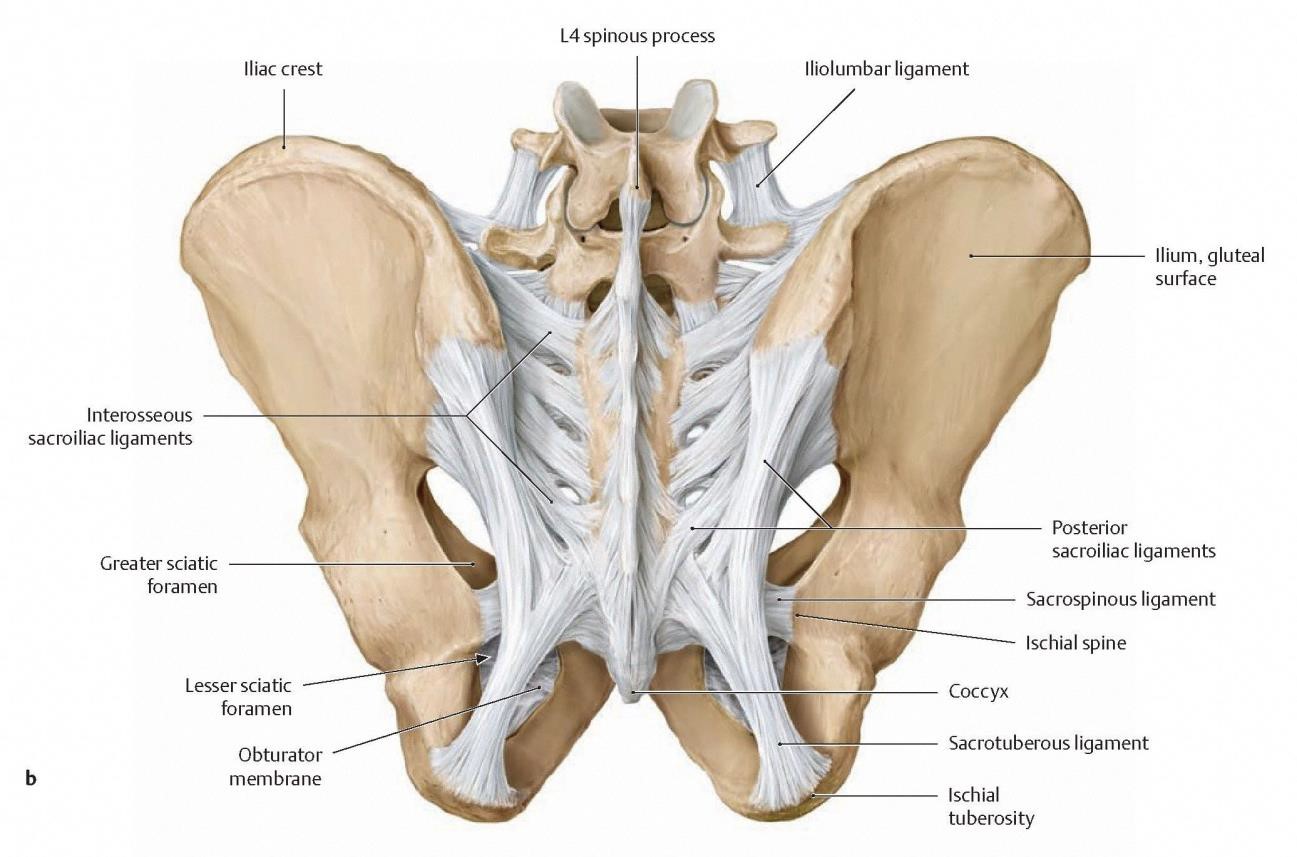
This ligament is the strongest stabilizer of the SI joint.
Interosseous SI ligament:
It’s one of the strongest ligaments in the entire body. It sits deep between the sacrum and ilium and acts like a massive shock absorber, basically binding the pelvis together so force from the legs can transfer efficiently to the spine.
Most commonly tested with the side-lying sacral distraction test (hard to isolate)
300
During lumbar left-sided rotation of L4 on L5, which facets are gapped and which are impacted?
Left Rotation of L4 on L5
Left facet: Gapped
Right facer: Impacted
300
Central canal stenosis symptoms typically improve with this movement, and what is the name of the condition when patients experience pain when they are not in the relief position?
What is lumbar flexion and Neurogenic claudication
Neurogenic claudication is leg pain, heaviness, numbness, or weakness caused by lumbar spinal stenosis compressing the nerve roots - typically during walking or standing.
Hallmark features:
Worse with standing and walking
Relief with sitting or lumbar flexion
Patients often lean forward (shopping cart sign)
Symptoms may be bilateral
300
This SI joint test cluster requires three or more positive provocation tests to significantly increase post-test probability of SI joint–related pain. What are these tests?
Answer: Laslett cluster
(Distraction, Compression, Thigh Thrust, Sacral Thrust, Gaenslen’s)
300
A 45-year-old desk worker presents with anterior thigh pain not past the knee and deep buttock discomfort. Lumbar flexion and extension are minimally painful. Femoral nerve tension test reproduces anterior thigh pain. Hip flexion and IR are full and pain-free. 3/5 SI provocation tests positive.
Primary pain generator?
Most appropriate early exercise strategy?
Upper lumbar radiculopathy (L2–L4)
Exercise: neural mobility within irritability limits (femoral nerve flossing)
Anterior thigh pain + femoral nerve tension test is the key to knowing this is likley an upper lumbar radiculopathy
400
These muscles have fascial continuity with the thoracolumbar fascia and contribute to SI joint force closure.
Gluteus maximus & Latissimus dorsi
400
The key structure that creates form closure at the SI joint
What are the irregular, interlocking ridges and grooves of the sacral and iliac articular surfaces.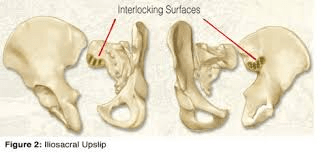
400
This disc pathology type involves nuclear material pushing out, but the annulus remains intact.
What is a disc protrusion (bulge)?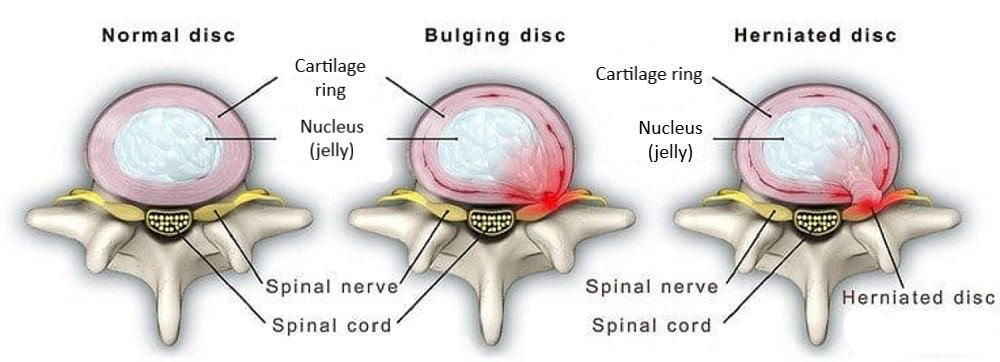
Disc Bulge
Broad, symmetrical extension of the disc beyond the vertebral body.
Annulus is stretched but usually intact.
Often age-related and may be asymptomatic.
Think: “disc is spilling out evenly.”
Disc Herniation
Focal displacement of nucleus pulposus through weakened annulus.
Can compress a nerve root.
Clinically:
Bulges are common and often incidental.
Herniations are more likely to be symptomatic, with radiculopathy.
400
Crossed Straight Leg Raise is highly specific but not sensitive. This means a positive test is useful for ruling in this condition.
Lumbar disc herniation with nerve root compression
What it indicates:
Strong sign of a large central or paracentral disc herniation
Significant nerve root irritation/compression
Often correlates with more severe pathology than a regular SLR
400
A 52-year-old runner presents with deep posterior buttock pain and intermittent groin discomfort. Pain is worse with prolonged sitting and with long runs. Lumbar repeated movements do not centralize or peripheralize symptoms. 3/5 SI provocation tests positive. Hip ROM shows mild IR restriction but no clear pain reproduction. FABER reproduces posterior buttock pain. SLR negative. Active straight leg raise improves with pelvic compression.
Primary pain generator?
Most appropriate early-stage management focus?
SI joint–related pain with impaired force closure
Load management + force closure strategy (deep abdominal activation, glute max, progressive single-leg stability)
500
In a posterolateral L4–L5 disc herniation, this nerve root is most commonly affected.
L5 nerve root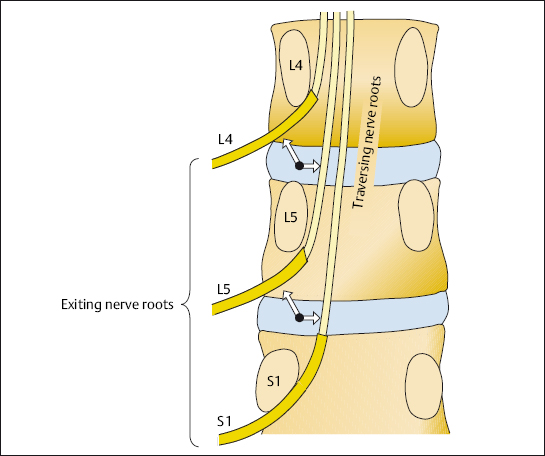
500
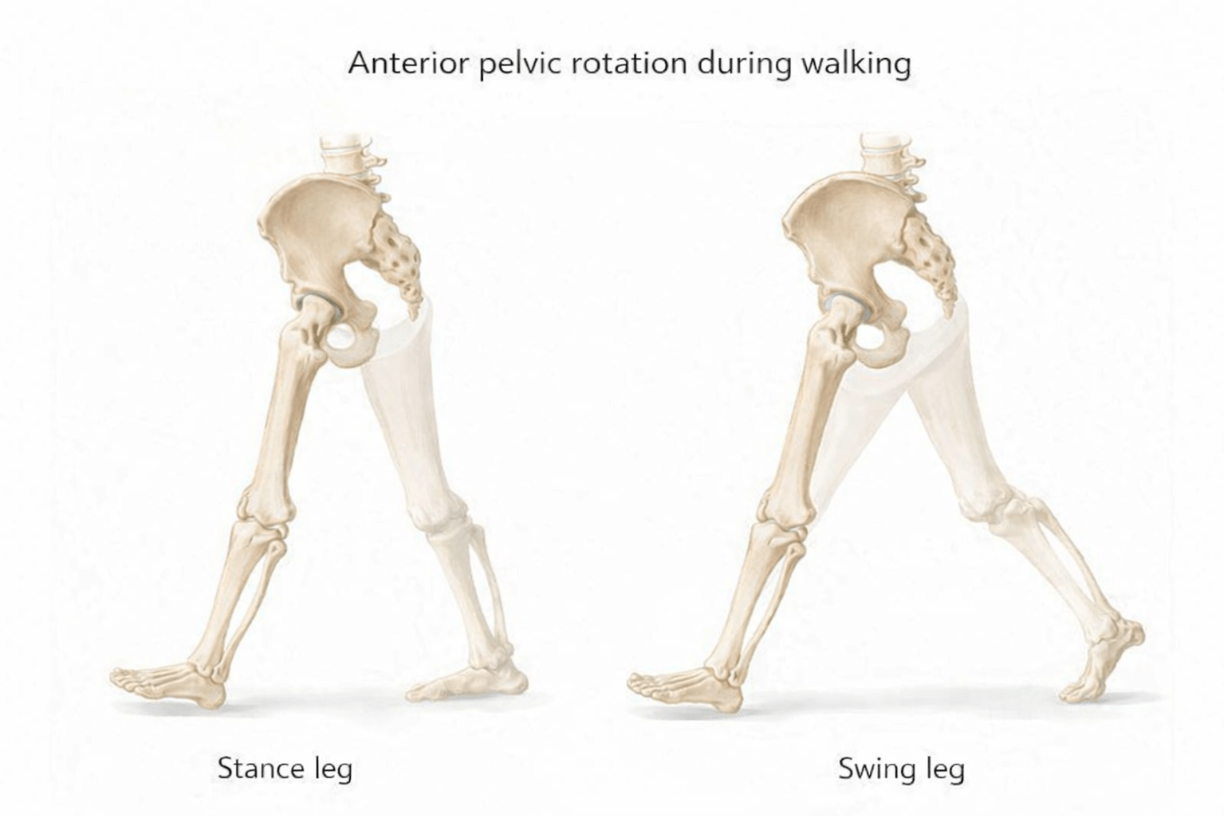
The movements that occur at the innominate during walking
During walking, the innominate bones move in a reciprocal and opposite pattern to accommodate hip motion.
-Stance leg innominate rotates anteriorly during hip extension
-The swing leg innominate rotates posteriorly during hip flexion , facilitating gait efficiency and weight transfer
So with right leg stance:
Right innominate = posterior rotation
Left innominate = anterior rotation
500
Patient presents with the following:
Deep, throbbing low back pain, doesn't really change with movement
Older male, smoker, vascular history
Possible pulsatile abdominal mass ((patient may describe “heartbeat in my stomach”)
What is your diagnosis?
Abdominal Aortic Aneurysm (AAA)
500
A patient presents with low back pain and leg symptoms.
Straight Leg Raise reproduces back pain only.
Slump test reproduces leg pain that increases with cervical flexion and decreases with cervical extension.
What does this pattern most strongly suggest?
Neural mechanosensitivity (radiculopathy) rather than hamstring tightness or purely local lumbar pain.
SLR reproducing only back pain is not strongly suggestive of radiculopathy.
Slump reproduces leg pain that changes with cervical movement, confirming neural involvement via structural differentiation.
Slump is more sensitive than SLR.
500
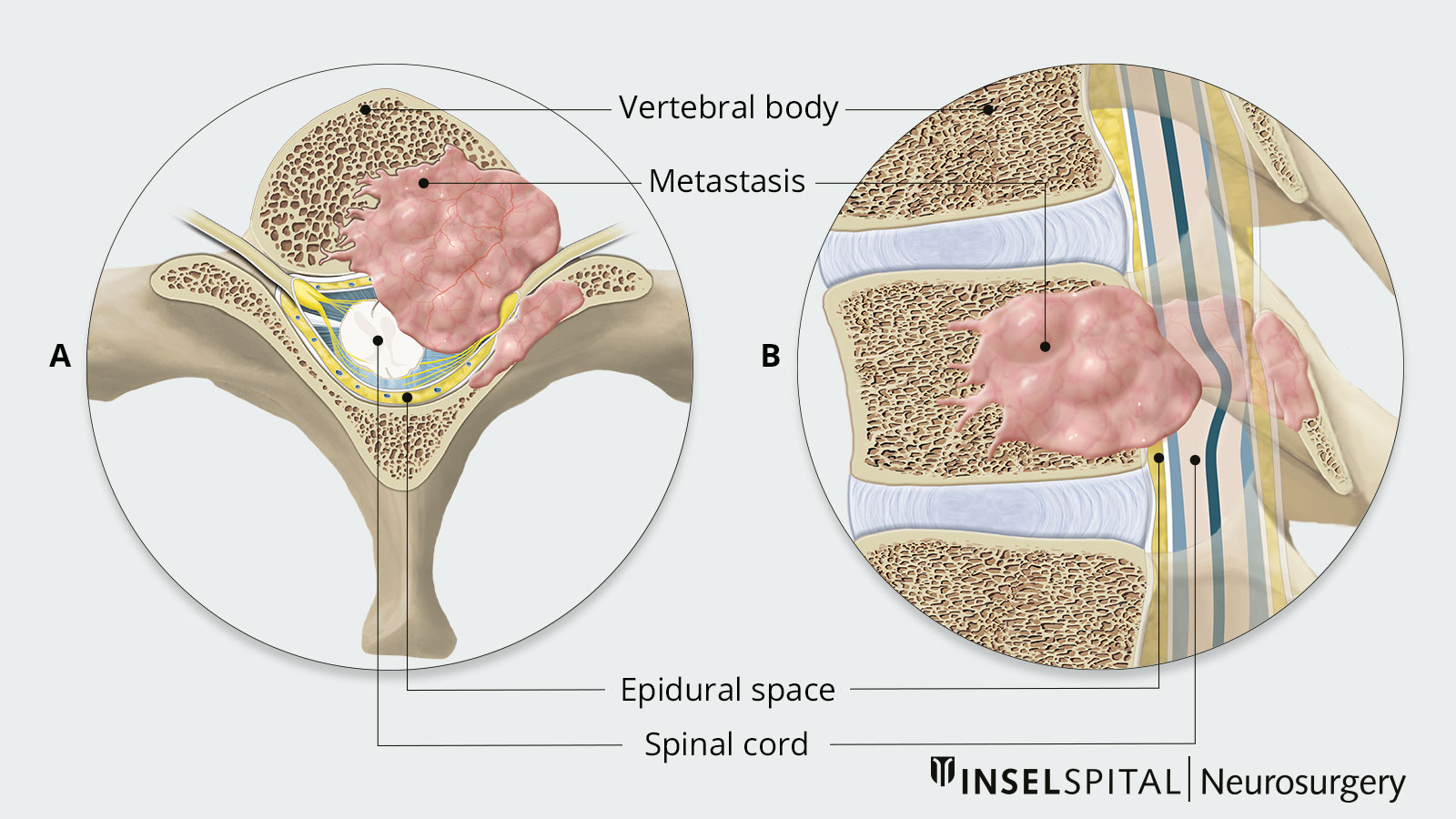
A 58-year-old male presents with progressively worsening low back pain over 6 weeks. He reports:
Constant, aching pain not relieved by rest
Pain worse at night and when lying supine
No clear mechanical aggravating or easing factors
no weight loss noted
History of prostate cancer 5 years ago (in remission)
Lumbar ROM is mildly limited but does not clearly reproduce his pain. Neuro screen is normal.
What is the most concerning underlying pathology?
What is the most appropriate immediate management step?
Suspected spinal metastasis (malignancy)
Immediate medical referral for imaging and physician evaluation (no exercise intervention)