Who ordered this?!
consult ID 🐛
The patient is trying to die 🏨
Rapid response roulette
Sick pics 😱
100
Hospitalized patient with ESRD becomes acutely encephalopathic and develops myoclonus after several days of antibiotics for Pseudomonas coverage. CT head is negative.
What medication toxicity is most likely occurring?
Cefepime neurotoxicity!
Cefepime neurotoxicity classically causes encephalopathy, aphasia, myoclonus, and seizures, especially in renal failure.
100
Patient admitted for COPD exacerbation has Candida growing in sputum culture. Broad-spectrum antifungal therapy is started overnight.
According to IDSA guidance, what is the most appropriate management?
No antifungal treatment is indicated.
-Candida in respiratory secretions almost always represents colonization, not Candida pneumonia.
100
Elderly hospitalized patient suddenly becomes confused, tachypneic, and difficult to arouse. Vitals: BP 86/52, RR 32, temp 39.4°C. Lactate is 6.8. Broad-spectrum antibiotics and IV fluids are initiated for septic shock.
According to current sepsis guidelines, what is the recommended initial crystalloid fluid dose?
30 ml/Kg.
Early aggressive crystalloid resuscitation is recommended for sepsis-induced hypoperfusion or septic shock.
100
TRUE or FALSE: A patient on warfarin with INR 2.4 who wakes up with new left hemiplegia and a negative CT head can still receive IV tPA if you reverse the INR below 1.7 with FFP before administering it.
FALSE. INR >1.7 at presentation is an absolute contraindication to tPA — you cannot 'reverse and retry.' FFP carries its own risks, and the time lost eliminates the treatment window. The right move: urgent neurology consult and evaluation for mechanical thrombectomy, which is eligible up to 24 hours in selected patients per DAWN/DEFUSE-3 criteria.
100
What is the treatment of this disease?

Oral terbifine!!
The other oral options have more side effects and the treatment is longer! First line treatment! topical antifungals ONLY if mild <50% surface of nail
200
Patient admitted for COPD exacerbation develops severe leukocytosis, insomnia, and acute delirium. You review the medication list with the intern who placed the orders.
What medication is the most likely cause?
Methylprednisolone!!
steroid-induced psychosis, it can occur at doses > 80mg/day
200
Blood cultures grow Staphylococcus aureus in 1 of 2 bottles in a patient with no fever and normal WBC count. The overnight resident documents “likely contaminant.”
What is the correct next step?
Treat as true bacteremia and repeat blood cultures.
-S. aureus bacteremia should never be automatically dismissed as contamination. Unlike:
- coagulase-negative staph (epidermidis)
- Corynebacterium
- Bacillus (non-anthracis)
200
Elderly patient admitted for pneumonia suddenly develops severe abdominal pain, profound distention, and rising lactate after several days of vasopressors in the ICU. CT abdomen is initially nonspecific and the abdominal exam seems “not that impressive.”
What catastrophic diagnosis should still be strongly suspected?
Mesenteric ischemia!!
Pain out of proportion to exam + lactic acidosis in a critically ill patient is bowel ischemia until proven otherwise.
In Early disease ct may have minimal findings
Non occlusive mesenteric ischemia (especially ICU/pressor patients) can have very subtle imaging. Clinical suspicion is critical
200
Rapid response called to the PCU. Patient with known cirrhosis was admitted with Hgb 2.3 and received 6 units of pRBCs. Now acutely hypoxic with O₂ sat 84% on room air. Stat chest X-ray shows the following. What is the diagnosis — and what is your immediate management?
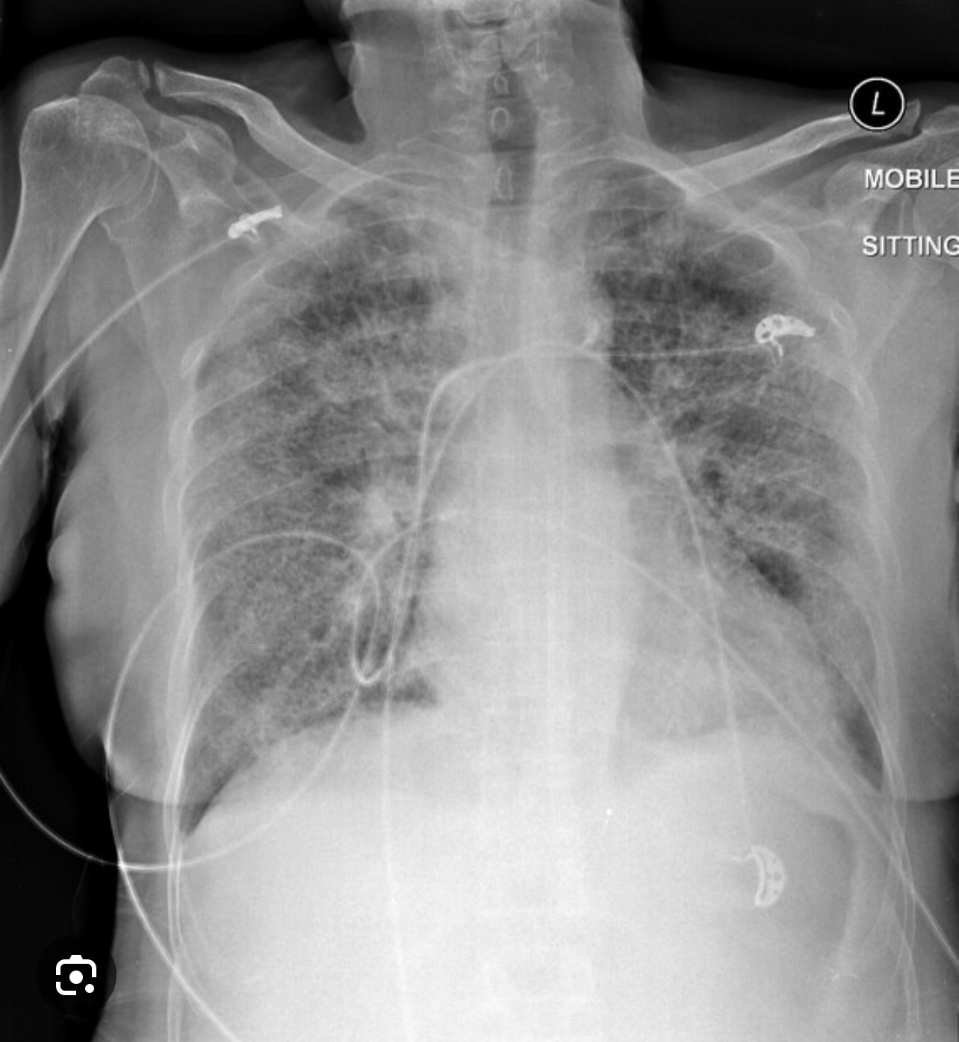
TRALI!!!
The X-ray shows bilateral patchy infiltrates WITHOUT cardiomegaly — classic non-cardiogenic pulmonary edema. The key distinguishing feature from TACO: no cardiomegaly, no pleural effusions, and hypotension (not hypertension). Immediate management: 1. STOP the transfusion immediately. Notify the blood bank to quarantine the donor unit and test for anti-HLA / anti-neutrophil antibodies. 2. Supportive oxygenation — high-flow O₂, escalate to HFNC or intubation if needed. 3. Low tidal volume ventilation if intubated (same ARDS strategy, 6 ml/kg IBW). 4. Do NOT give diuretics — this is non-cardiogenic edema; diuretics can worsen hypotension. 5. Most patients recover in 48–96 hours with supportive care.
200
Patient on Minocycline for rosacea developed blue-gray discoloration of the skin.
What adverse effect is shown in this image?

Minocycline-induced hyperpigmentation.
Long-term minocycline use can deposit pigment in the skin, nails, gums, and scars, causing characteristic blue-gray discoloration. Only if taking it for months! It can go away by stopping the med but takes time.
300
Intubated ICU patient with severe ARDS has been deeply sedated for several days. The nurse called you at bedside for sudden bradycardia, worsening vasopressor requirements, and refractory high anion gap metabolic acidosis despite adequate oxygenation and negative infectious workup. Labs later reveal CK 18,000 and triglycerides 1,200.
What medication-related syndrome should be immediately suspected?
Propofol infusion syndrome.
Prolonged/high-dose Propofol can cause mitochondrial dysfunction leading to metabolic acidosis, rhabdomyolysis, hypertriglyceridemia, arrhythmias, and cardiovascular collapse.
300
Dairy farmer admitted to the hospital for prosthetic valve endocarditis has persistently negative blood cultures despite ongoing fevers and embolic strokes. Serologies later return positive.
What organism is the most likely cause?
Brucellosis!!!
Brucella is a classic cause of culture-negative endocarditis associated with livestock exposure and unpasteurized dairy products.
Others: hacek, coxiella, bartonella, Tropheryma whipplei, candida, aspergillus, Libman-Sacks
300
Rapid response called for sudden hypoxia and altered mental status in a patient admitted for severe acute pancreatitis. Patient is tachycardic, confused, requiring escalating oxygen, and develops a new petechial rash over the chest and axilla. CTA chest is negative for PE.
What life-threatening complication should be suspected?
Fat embolism!
Classic causes Long bone fractures (most common), Orthopedic trauma/surgery, Acute pancreatitis, Liposuction/burns (less common).
Classic Triad: Hypoxemia/respiratory, neurological sx and petechial rash!
300
75 y/o man with DM on glipizide admitted for UTI and AKI. Rapid response called for altered mental status. Fingerstick glucose is 25. After IV dextrose, repeat glucose remains 35.
What medication should be given to prevent further recurrent hypoglycemia?
Octeotride!!!
Sulfonylureas cause persistent endogenous insulin release. Specially prolonged in AKI. octeotride supresses insulin secretion and helps prevent rebound hypoglycemia
300
This ophthalmologic condition, characterized by rubbery “floppy” eyelids and chronic conjunctivitis, is strongly associated with what common disorder?
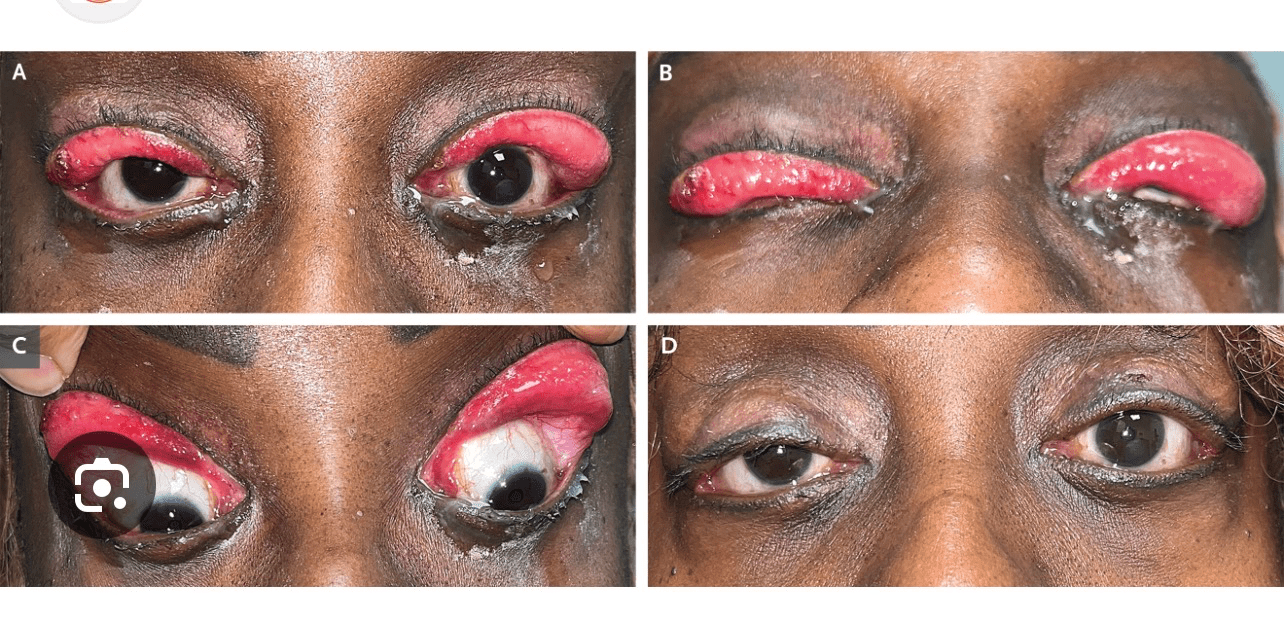
Obstructive sleep apnea!!!
floppy eyelid syndrome! This syndrome is characterized by excessive laxity of the upper eyelids and results in eyelid malposition and chronic irritation of the ocular surface. It is associated with obstructive sleep apnea.
Treatment cpap, ophthalmic lubricants, and eye patches while sleeping.
400
45 y/o woman from a group home with PMH of schizophrenia is admitted for VRE bacteremia and treated with IV Linezolid. By hospital day 3 she is clinically improving, so her home psychiatric medications are resumed. The following day, she develops severe agitation, diaphoresis, inducible clonus, hyperreflexia, hyperthermia, and marked hypertension. CT head and repeat cultures are unrevealing. You review the medication list and identify the culprit interaction.
What does this patient have?
Serotonin syndrome!!!
Classic Triad: Mental status changes, Autonomic instability (tachy, diaphoresis), Neuromuscular hyperactivity (clonus, hyperreflexia, rigidity, tremors)
This patient was given linezolid and resumes her psych home meds!
Linezolid has monoamine oxidase inhibitor (MAOI) activity. Mao breaks down serotonin. Be careful when using linezolid with psych meds and sedation in the icu
400
Patient with uncontrolled diabetes is admitted for DKA and initially improves with insulin therapy. Two days later, rapid response is called for worsening facial pain, acute confusion, diplopia, and unilateral ophthalmoplegia. Exam reveals a black necrotic lesion on the hard palate. MRI demonstrates invasive fungal sinusitis with orbital extension.
What is the most important next step in management in addition to antifungal therapy?
Emergent surgical debridement.
Rhinocerebral mucormycosis is angioinvasive and rapidly necrotizing. Survival depends on early aggressive surgical debridement plus IV amphotericin B.
400
COPD patient admitted for HF exacerbation is receiving IV diuresis. Family increases his oxygen to 15 L overnight because he “looked uncomfortable.” Rapid response is called the next morning for worsening somnolence.
ABG: pH 7.36 / pCO₂ 78 / HCO₃⁻ 43 / pO₂ 198
What is the acid-base disorder?
Chronic respiratory acidosis with superimposed metabolic alkalosis.
For chronic respiratory acidosis bicarbonate should increase about 4 for every 10 rise in pCO2. This patient has pco2 78
4 times 4 = 16
Expected HCO₃⁻:
24 + 16 = 40
If measured HCO₃⁻ is significantly higher (like 43), then there is an additional metabolic alkalosis
400
Rapid response called after a previously calm hospitalized patient suddenly becomes severely agitated, hallucinating, pulling at lines, and trying to climb out of bed. He has hx of parkinson and is admitted for pna. The nurse is screaming at you for a prn med.
What medication should generally be avoided?
Haloperidol!
Dopamine blockade can dramatically worsen parkinsonism and precipitate rigidity or neuroleptic sensitivity.
Safer options for agitation/delirium in Parkinson disease:
- Quetiapine
- Sometimes benzodiazepines depending on the cause
400

This characteristic rash, called larva currens, is a clue to disseminated infection by what parasite, especially in immunosuppressed patients?
Strongyloidiasis!
Larva currens is a fast-moving serpiginous rash caused by autoinfection from Strongyloidiasis and can become fatal in immunosuppressed patients
500
patient admitted for severe alcohol withdrawal remains profoundly agitated despite escalating doses of continuous Lorazepam infusion. On hospital day 4, rapid response is called for worsening shock, unexplained high anion gap metabolic acidosis, AKI, and rising osmolar gap.
What ICU-related medication toxicity should be suspected?
Propylene glycol toxicity.
IV lorazepam does not dissolve well in water so propylene glycol is use as a solvent. At risk only iv formulation and continous drips.
Propylene glycol is metabolized into organic acids (including lactate), which accumulate and increase the anion gap and osmolar gap.
The osmolar gap is calculated by comparing the measured serum osmolality to the calculated serum osmolality. If high think of methanol, ethylene glycol, isopropyl alcohol, propylene glycol,mannitol
500
Patient recently returned from rural Central/South America and reports a painful “pimple” sensation with intermittent movement inside the lesion.
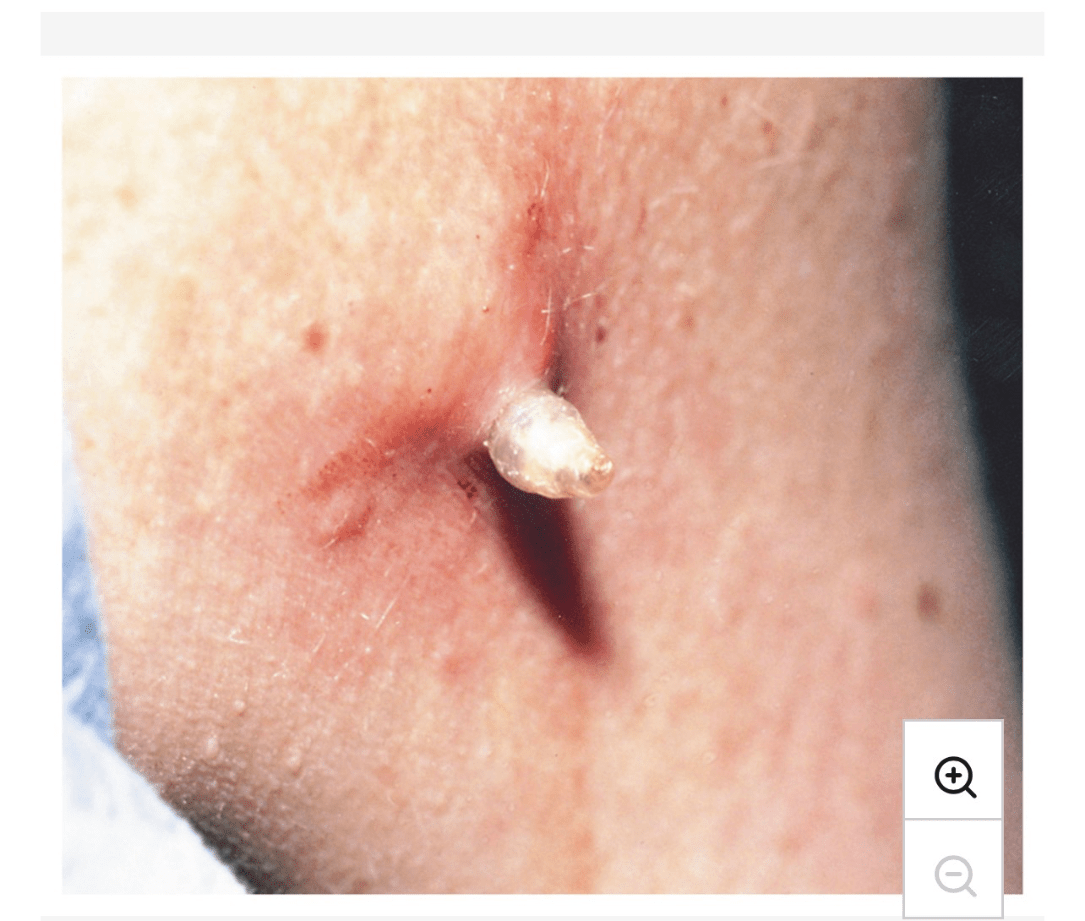
What parasitic infection is shown in this image?
Furuncular myiasis.
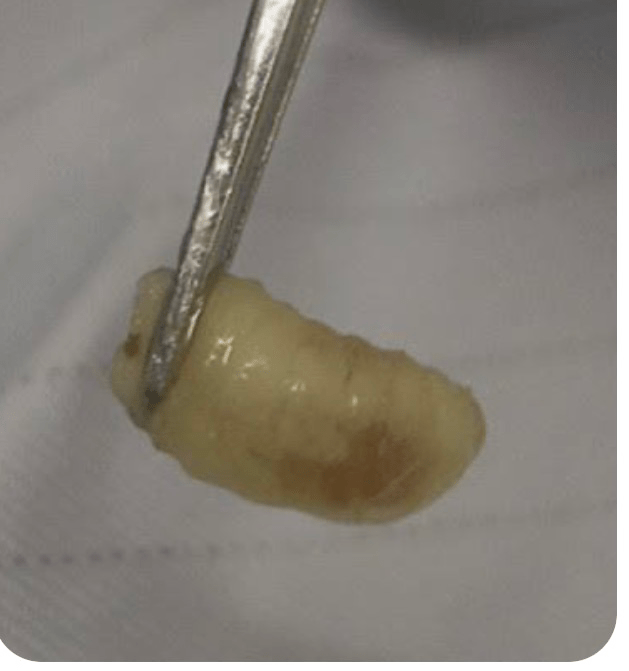 Parasitic infection from fly larvae.
Parasitic infection from fly larvae.
Patients develops
- painful furuncle-like lesion
- central punctum
- serous drainage
- sensation of movement or “something alive”
- intermittent sharp pain
500
Urology does a direct admit for planned right radical nephrectomy and IVC thrombectomy but then calls you to take primary because now the patient is “more medical.” On the way upstairs to see the patient, a rapid response is called with no admission orders placed yet.
Patient has severe abdominal pain, jaundice, lower extremity edema, and tense ascites with positive fluid wave on exam. Labs show markedly elevated LFTs, and ultrasound demonstrates hepatic venous outflow obstruction.
What complication has this patient developed?
Budd-Chiari syndrome
Think Budd-Chiari in a patient with:
- ascites + liver injury + abdominal pain
- especially with hypercoagulability (Factor V Leiden,antiphospholipid syndrome)
- or RCC involving the IVC.
500
Rapid response called for acute altered mental status. You quickly check his chart. He is here for alcohol withdrawal. His electrolytes are normal and vs were good besides some tachycardia. Now his tele is showing this and the nurse is pushing the botton for code blue.
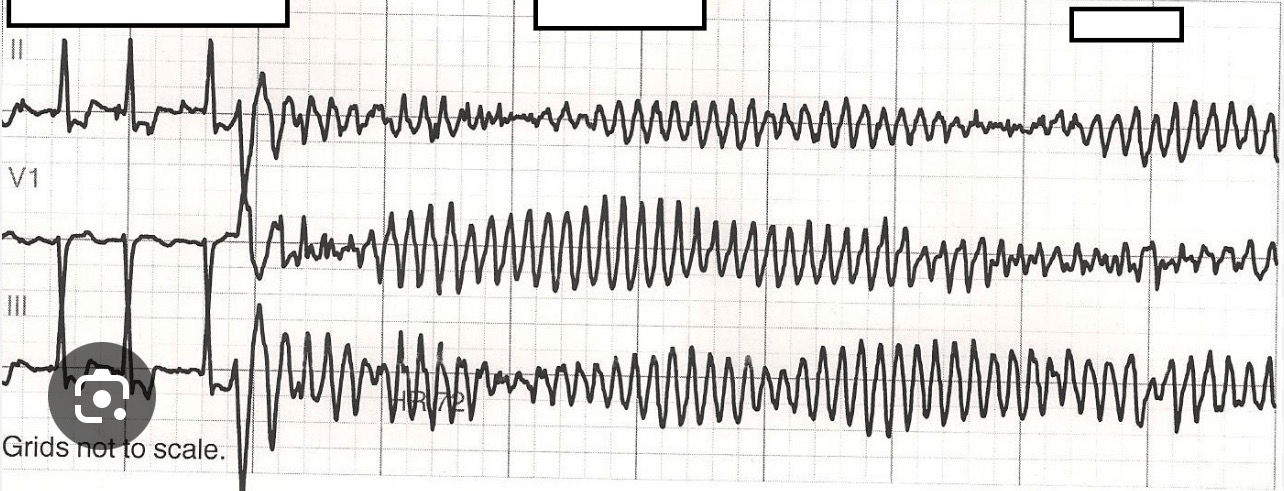
What is the first-line treatment?
IV Magnesium sulfate.
Magnesium is first-line therapy for torsades even if the serum magnesium level is normal.
500
22 y/o M with pmh kidney stones and recent UTI 2 weeks ago comes for f/u Microscopic examination of a spun urine specimen is shown, demonstrating two crystal types. What are these crystals?
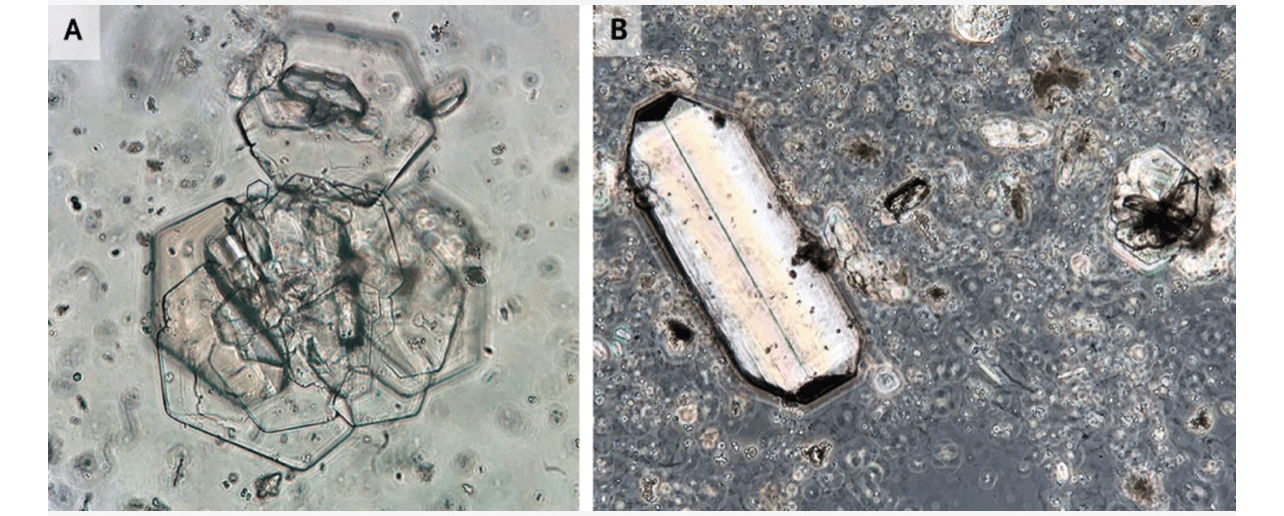
cystine and triple phosphate (struvite) crystals!
- Coffin = struvite
- Hexagon = cystine
- Envelope = oxalate
- Diamond = uric acid
- Calcium phosphate = Starburst/rosettes