respiratory
vent
hemodynamics
shock
burns
100
A patient asks, “How does air get into my lungs?” The nurse bases her answer on knowledge that air moves into the lungs because of
a. positive intrathoracic pressure.
b. contraction of the accessory abdominal muscles.
c. stimulation of the respiratory muscles by the chemoreceptors.
d. a decrease in intrathoracic pressure from an increase in thoracic cavity size.
d. a decrease in intrathoracic pressure from an increase in thoracic cavity size.
The diaphragm is the major muscle of respiration. During inspiration the diaphragm contracts, moves downward, and increases intrathoracic volume. At the same time, the internal intercostals relax and the external intercostal muscles contract. This increases the lateral and anteroposterior (AP) dimension of the chest.
The scalene muscles also contract on inspiration, raising the first and second ribs. This causes the size of the thoracic cavity to increase and intrathoracic pressure to decrease, pulling air into the lungs.
100
After endotracheal intubation & mechanical ventilation have been started, a pt in respiratory failure becomes very agitated and is breathing asynchronously with the vent. What is most important for the nurse to do first?
a. evaluate the pt's pain level, ABG, & electrolyte values
b. sedate the pt to unconsciousness to eliminate pt awareness
c. give as needed vecuronium to promote synchronous ventilations
d. slow the ventilator rate of ventilations to allow for the pt to spontaneously breathe.
a. evaluate the pt's pain level, ABG, & electrolyte values
Tx underlying cause before sedating pt - giving more drugs could prolong hospitalization
Analgesia and sedation, either by direct IV or continuous IV infusion, are important. Analgesia and sedation decrease the discomfort associated with the presence of an ET tube, help reduce WOB, and prevent ventilator dyssynchrony.
100
What do you know about Preload?
What do you know about Afterload?
Volume within the ventricle at the end of diastole
Think of preload as "fluid vol status of pt"
CVP R side heart preload (2-8); PAWP (8-12) & PAP (15-25) L side heart preload
If preload high= pump failure, heart failure, fluid vol overload
If preload low= fluid vol deficit, dehydration from vomiting/diarrhea, bleeding profusely; vasodilation
Forces opposing ventricular ejection or resistance the heart has to overcome to pump
"vessel diameter"
SVR (800-1200) L side of heart afterload; PVR (0.25-1.6) R side of heart afterload
If afterload high= vasoconstriction, hypothermic, raas system activated
If afterload low= vasodilation, infection, inflammation, hyperthermia
garden hose vs fire hose analogy
100
Progressive tissue hypoxia leading to anaerobic metabolism and metabolic acidosis is characteristic of the progressive stage of shock. What changes in the heart contribute to tissue hypoxia?
a. Coronary artery constriction causes decreased perfusion.
b. Cardiac vasoconstriction decreases blood flow to pulmonary capillaries.
c. Increased capillary permeability and profound vasoconstriction cause increased hydrostatic pressure.
d. Decreased perfusion occurs, leading to dysrhythmias, decreased CO, and decreased oxygen delivery to cells.
d. Decreased perfusion occurs, leading to dysrhythmias, decreased CO, and decreased oxygen delivery to cells.
table 66.5 or table 42.5
The progressive stage of shock begins as compensatory mechanisms fail. Changes in the patient’s mental status are important findings in this stage. Patients must be moved to the intensive care unit (ICU), if not already there, for advanced monitoring and treatment.
The cardiovascular system is profoundly affected in the progressive stage of shock. CO begins to fall, resulting in a decrease in BP and coronary artery, cerebral, and peripheral perfusion. Continued decreased cellular perfusion and resulting altered capillary permeability are the distinguishing features of this stage. Altered capillary permeability allows fluid and protein to leak out of the vascular space into the surrounding interstitial space. In addition to the decrease in circulating volume, there is an increase in systemic interstitial edema. The patient may have anasarca (diffuse profound edema). Fluid leakage from the vascular space affects the solid organs (e.g., liver, spleen, GI tract, lungs) and peripheral tissues by further decreasing perfusion.
Decreased myocardial perfusion leads to dysrhythmias and myocardial ischemia, further decreasing CO and oxygen delivery to cells.
The kidney’s renin-angiotensin-aldosterone system activation causes arteriolar constriction that decreases perfusion.
In the lung, vasoconstriction of arterioles decreases blood flow and a ventilation-perfusion mismatch occurs. Areas of the lung that are oxygenated are not perfused because of the decreased blood flow, resulting in hypoxemia and decreased oxygen for cells.
Increased capillary permeability and vasoconstriction cause increased hydrostatic pressure that contributes to the fluid shifting to interstitial spaces, but this is not a change in the heart.
100
When assessing a patient with a partial-thickness burn, the nurse would expect to find (select all that apply)
a. blisters.
b. exposed fascia.
c. exposed muscles.
d. intact nerve endings.
e. red, shiny, wet appearance.
a. blisters.
d. intact nerve endings.
e. red, shiny, wet appearance.
table 24.5 or table 26.4
https://img.grepmed.com/uploads/12028/burn-grading-classification-diagnosis-degrees-2200w.jpeg
Partial thickness or 1st deg burns appearance: Erythema, blanching on pressure, pain and mild swelling, no vesicles or blisters (although after 24 hr skin may blister and peel)
Deep thickness or 2nd deg burns appearance: Fluid-filled vesicles that are red, shiny, wet (if vesicles have ruptured). Severe pain caused by nerve injury. Mild to moderate edema
fig 24.3 or fig. 26.3: full thickness burns (3rd-4th deg burns) would see exposed fat, muscle or bone
200
Which descriptions are characteristic of hypoxemic respiratory failure (select all that apply)?
a. referred to as a ventilatory failure
b. main problem is inadequate O2 transfer
c. risk of inadequate O2 saturation of hemoglobin exists
d. body is unable to compensate for acidemia of increased partial pressure of carbon dioxide in arterial blood
e. most often caused by ventilation perfusion (V/Q) mismatch & shunt
f. exists when partial pressure of oxygen in arterial blood (PaO2) is less than 60 mmHg, even when O2 is given at 60% or more
b. main problem is inadequate O2 transfer
c. risk of inadequate O2 saturation of hemoglobin exists
e. most often caused by ventilation perfusion (V/Q) mismatch & shunt
f. exists when partial pressure of oxygen in arterial blood (PaO2) is less than 60 mmHg, even when O2 is given at 60% or more
Hypoxemic = oxygen failure: inadequate oxygen transfer, inadequate oxygen saturation of hemoglobin; V/Q mismatch (fig. 67.3 or fig. 32.3) & shunt (blood exits the heart without having taken part in gas exchange)
In normal lungs, the volume of blood perfusing the lungs and the amount of gas reaching the alveoli are almost identical. So, when you compare normal alveolar ventilation (4 to 6 L/min) to pulmonary blood flow (4 to 6 L/min), you have a V/Q ratio of 0.8 to 1.2.
In a perfect match, ventilation and perfusion would yield a V/Q ratio of 1:1, expressed as V/Q = 1. When the match is not 1:1, a V/Q mismatch occurs. V/Q ratios > 1 (more ventilation than perfusion). V/Q ratios < 1 (less ventilation than perfusion).
The most common problems that cause a V/Q mismatch are those in which increased secretions are present in the airways (e.g., COPD) or alveoli (e.g., pneumonia) or bronchospasm is present (e.g., asthma). V/Q mismatch may result from pain, alveolar collapse (atelectasis), or pulmonary emboli. The best way to treat hypoxemia caused by a V/Q mismatch is to treat the cause.
Hypercapnic respiratory failure (or ventilatory failure) is a PaCO2 greater than 50 mm Hg with acidemia (arterial pH less than 7.35).
choice a, d = hypercapnic or ventilatory failure
200
When mechanical ventilation is used for the pt with ARDS, what is the reason for applying PEEP?
a. prevent alveolar collapse & open collapsed alveoli
b. permit smaller tidal volume with permissive hypercapnia
c. promote complete emptying of the lungs during exhalation
d. permit extracorporeal oxygenation and carbon dioxide removal outside the body
a. prevent alveolar collapse & open collapsed alveoli
Positive End Expiratory Pressure increases functional residual capacity, or the volume of air left in the lungs at the end of a normal expiration. PEEP also helps open up (or “recruit”) collapsed alveoli.
We typically apply PEEP in increments of 3 to 5 cm H2O until oxygenation is adequate, with an FIO2 of 60% or less (if possible). PEEP may improve ventilation in respiratory units that collapse at low airway pressures, thus allowing the FIO2 to be lowered.
Patients with ARDS may need higher levels of PEEP (e.g., 10 to 20 cm H2O). There is no identified optimal level of PEEP for patients with ARDS.
The added intrathoracic and intrapulmonic pressures generated by positive pressure remaining in the lungs and transmitted to surrounding structures (e.g., inferior vena cava, heart) at end expiration can compromise venous return. This in turn has the potential to decrease the amount of blood returning to both the right and left sides of the heart. Dramatic reductions in preload, CO, and BP can occur. High levels of PEEP or excess inspiratory pressures can cause barotrauma and volutrauma.
choice b is a treatment option for ARDS, but does not pertain to PEEP and is used in pts with who have smaller tidal volumes to prevent barotrauma
choice c word usage of promote "complete emptying" of the lungs during exhalation is not accurate
choice d = ECMO
The primary goal of O2 therapy is to correct hypoxemia. As respiratory failure worsens, high-flow O2 will be not be able to keep the PaO2 within acceptable ranges.
Mechanical ventilation is often delivered via a pressure-control type of ventilation. Pressure-control ventilation helps to keep the inspiratory and plateau pressures from becoming too high. This prevents alveolar overdistention and rupture. By reducing the amount of pressure going into the stiff, noncompliant lungs, we can help prevent further lung injury.
table 67.9 or table 32.9
200
During hemodynamic monitoring, the nurse finds that the patient has a decreased CO with unchanged pulmonary artery wedge pressure (PAWP), HR, and SVR. What would the nurse identify has decreased?
a) Preload
b) Afterload
c) Contractility
d) Stroke Volume
c) Contractility
Cardiac Output is dependent upon Heart Rate and Stroke Volume. CO = HR x SV
Stroke Volume is determined by preload, afterload, and contractility.
If Cardiac Output is decreased and Heart Rate is unchanged, Stroke Volume is the variable factor.
If the preload (PAWP) and afterload (SVR) are unchanged, the factor that is changed is the contractility of the myocardium.
200
Hemodynamic pattern of hypovolemic shock
preload= low
contractility= low
afterload= high
Pt is anxious, low UOP (low tissue perfusion): treat the cause - O2 prn, give crystalloid isotonic IV fluid replacement to keep fluid in intravascular space to increase intravascular volume; position pt supine with feet elevated with hob flat or < 30; warm IV fluids; monitor UOP, cardiac tele, labs, abg
200
A patient is admitted to the burn center with burns to his head, neck, and anterior and posterior chest after an explosion in his garage. On assessment, the nurse auscultates wheezes throughout the lung fields. On reassessment, the wheezes are gone, and the breath sounds are greatly decreased. Which action is the most appropriate for the nurse to take next?
a. Encourage the patient to cough and auscultate the lungs again.
b. Obtain vital signs, oxygen saturation, and a STAT arterial blood gas.
c. Document the findings and continue to monitor the patient’s breathing.
d. Anticipate the need for endotracheal intubation and notify the provider.
d. Anticipate the need for endotracheal intubation and notify the provider.
Decreased or absent breath sounds may signal a significant decrease in air movement resulting from exhaustion and an inability to generate enough muscle force to breathe.
Severely decreased breath sounds, often referred to as the “silent chest,” are an ominous sign. It means severe airway obstruction and impending respiratory failure.
300
Which patient with the following manifestations is most likely to develop hypercapnic respiratory failure?
a. rapid, deep respirations in response to pna
b. slow, shallow respirations because of sedative overdose
c. large airway resistance because of severe bronchospasm
d. poorly ventilated areas of the lung due to pulmonary edema
b. slow, shallow respirations because of sedative overdose
Associated with alveolar hypoventilation with increases in alveolar and arterial CO2 and often is caused by problems outside the lungs.
This slow shallow resp are not exchanging enough gas vol to eliminate CO2
The other choices a, c, & d: correlate with hypoxemic (oxygenation) respiratory failure
300
How do nurses prevent acidosis complications in pts who are receiving mechanical ventilation?
Assess vent settings (may have alveolar hypoventilation causing retention of CO2; low tidal vol or low resp rate)
Leakage of air from vent tubing (lower tidal vol)
Lung secretions or obstruction (sxn); cough deep breathing; pulmonary toileting
Therefore: increase tidal volume or resp rate & consider adding small amts of PEEP
300
BP 78/44; CVP= 2 (normal), SVR= 400 (low)
a. nitrate
b. fluids
c. ionotrope/constrictor
d. diuretic
b. fluids
Follow up with pressor if needed after filling up the tank
300
70 yo pt with malnourishment & hx of DM2 is admitted from the nursing home with pna and tachypnea. Which kind of shock is this pt most likely to develop?
a. septic shock
b. obstructive shock
c. cardiogenic shock
d. anaphylactic shock
a. septic shock
Pt may present with fever, hypothermia, increased hr, increased rr, ams, significant edema, or hyperglycemia without dm are all criteria for dx of sepsis
Tx septic shock- aggressive IV fluids isotonic crystalloids; antibiotics as ordered; vasopressor; ionotrope; anticoagulant (lovenox); obtain cultures before starting antibiotics - monitor temp & blood glucose checks - prevent stress ulcer formation
Obstructive shock develops when a physical obstruction to blood flow occurs with a decreased CO. Patients have a decreased CO, increased afterload, and variable left ventricular filling pressures depending on the obstruction. Other signs include jugular venous distention and pulsus paradoxus (Pulsus paradoxus = a decrease in the systolic blood pressure during inspiration, results from a decrease in cardiac stroke volume with inspiration due to greatly increased left-ventricular afterload).
300
Pain management for the burn patient is most effective when (select all that apply)
a. a pain rating tool is used to monitor the patient’s level of pain.
b. painful dressing changes are delayed until the patient’s pain is completely relieved.
c. the patient is informed about and has some control over the management of the pain.
d. a multimodal approach is used (e.g., sustained-release and short-acting opioids, NSAIDs, adjuvant analgesics).
e. nonpharmacologic therapies (e.g., music therapy, distraction) replace opioids in the rehabilitation phase of a burn injury.
a. a pain rating tool is used to monitor the patient’s level of pain.
c. the patient is informed about and has some control over the management of the pain.
d. a multimodal approach is used (e.g., sustained-release and short-acting opioids, NSAIDs, adjuvant analgesics).
choice b = pain may not be completely relieved, tx pain with opioids and/or combo of other meds
choice e = possible to consider, depending on the pt and their progress: The formal rehabilitation phase begins when the patient’s wounds have nearly healed and they are engaging in some level of self-care. This may happen as early as 2 weeks or as long as 7 to 8 months after a major burn injury. Base ongoing pain management and nutritional needs on individual patient status. Continue to encourage the patient to perform the PT and OT routines. Encourage and reassure the patient to maintain morale, particularly once the patient realizes that recovery can be slow. Rehabilitation may have to be a primary focus for at least the next 6 to 12 months.
400
The most common early clinical manifestations of ARDS that the nurse may see are
a. dyspnea and tachypnea.
b. cyanosis and apprehension.
c. respiratory distress and frothy sputum.
d. bradycardia and increased work of breathing
a. dyspnea and tachypnea.
Acute Respiratory Distress Syndrome is a sudden and progressive form of Acute Respiratory Failure in which the alveolar-capillary membrane becomes damaged and more permeable to intravascular fluid; mc cause = sepsis
The injury or exudative phase usually occurs 24 to 72 hours after the initial insult (direct or indirect). It generally lasts up to 7 days.
Engorgement of the peribronchial and perivascular interstitial space causes interstitial edema. Fluid in the parenchyma of the lung surrounding the alveoli crosses the alveolar membrane and enters the alveolar space. V/Q mismatch and intrapulmonary shunt develop because the alveoli fill with fluid. Blood in the capillary network cannot be oxygenated.
At the time of the initial injury, and for 24 to 72 hours, the patient may not have respiratory symptoms or may have only mild dyspnea, tachypnea, cough, and restlessness.
Lung auscultation may be normal or reveal fine, scattered crackles.
ABGs may show mild hypoxemia and respiratory alkalosis caused by hyperventilation.
The chest x-ray may be normal or reveal diffusely scattered, but minimal, interstitial infiltrates.
400
In caring for a pt in acute respiratory failure, the rn recognizes that noninvasive positive pressure ventilation may be used for which pt?
a. is comatose and has high O2 requirements
b. has copious secretions that require frequent suctioning
c. responds to hourly bronchodilator neb treatments
d. is alert & cooperative but has increasing respiratory exhaustion
d. is alert & cooperative but has increasing respiratory exhaustion
Acute respiratory failure (ARF) occurs when oxygenation, ventilation, or both are inadequate. ARF is not a disease. It is a symptom that reflects lung function.
Non-Invasive Positive Pressure Ventilation (CPAP/BIPAP) is not appropriate for patients who have a decreased level of consciousness, high O2 requirements, facial trauma, hemodynamic instability, or excessive secretions. NIPPV used after extubation can help avoid reintubation.
choice a = not able to protect airway & has high oxygen requirements
choice b = possibly not able to protect airway, frequent suction needs don't go well with NIPPV
400
BP= 134/80, CO= 2 (low), CVP= 26 (high)
a. nitrate
b. fluids
c. ionotrope/constrictor
d. diuretic
a. nitrate
Need to decrease preload and afterload to improve co, bp should be able to tolerate nitrate
400
Treatment considerations for anaphylactic shock
Maintain patent airway
Optimize oxygenation
Intubate/ventilate if needed
IV fluids
Drugs to consider:
First line: Epinephrine (IM or IV): It causes peripheral vasoconstriction and bronchodilation and opposes the effect of histamine.
Antihistamines (e.g., diphenhydramine) - blocks histamine
Histamine (H2)-receptor blockers (e.g., ranitidine [Zantac]) - blocks histamine
Bronchodilators: nebulized (e.g., albuterol)
Corticosteroids (if hypotension persists)
preload = low
co = low
afterload = low
400
Number the following actions in the order they should be done in the emergency management of a burn of any type, beginning with #1 for the first action:
__ a. establish & maintain an airway
__ b. assess for other associated injuries
__ c. establish an IV line with a large gauge needle
__ d. remove the pt from the burn source & stop the burning process
a. 2
b. 4
c. 3
d. 1
At the scene of the injury, priority is given to removing the person from the source of the burn and stopping the burning process. Rescuers must protect themselves from being injured. In the case of electrical and chemical injuries, initial care involves removing the patient from contact with the electrical or chemical source.
If the burn is large (greater than 10% TBSA) or an electrical or inhalation burn is suspected, and the patient is UNRESPONSIVE, first focus your attention on CAB:
- Circulation: Check for presence of pulses and elevate the burned limb(s) above the heart to decrease pain and swelling.
- Airway: Check for patency, soot around nares and on the tongue, singed nasal hair, darkened oral or nasal membranes.
- Breathing: Check for adequacy of ventilation.
If the patient IS RESPONSIVE, your priorities would follow the order of the ABCs: airway, breathing, and circulation.
The emergent (resuscitative) phase is the time needed to resolve the immediate, life-threatening problems resulting from the burn injury. This phase usually lasts up to 72 hours from the time the burn occurred. The main concerns are the onset of hypovolemic shock and edema formation.
500
Interventions used in managing the patient with ARDS include (select all that apply)
a. IV injection of surfactant.
b. aggressive IV fluid resuscitation.
c. giving adequate analgesia and sedation.
d. elevating the head of bed 30 to 45 degrees when supine.
e. monitoring hemodynamic parameters and daily weights.
c. giving adequate analgesia and sedation.
d. elevating the head of bed 30 to 45 degrees when supine.
e. monitoring hemodynamic parameters and daily weights.
(table 67.9 or table 32.9)
Analgesia and sedation decrease the discomfort associated with the presence of an ET tube, help reduce WOB, and prevent ventilator dyssynchrony.
Elevate the HOB 30-45 when supine to allow for better lung expansion/ventilatory effort.
Patients with ARDS are at risk for hemodynamic compromise. Those on PPV and PEEP often have decreased CO. Hemodynamic monitoring (e.g., CVP, CO, ScvO2, SvO2) is essential. This allows you to see trends, detect changes, and adjust therapy as needed. BP and mean arterial pressure (MAP) are important indicators of the adequacy of CO.
Monitor hemodynamic parameters (e.g., CVP, stroke volume variation) and daily weights to assess the patient’s fluid volume status. Monitor intake and output hourly. Keep the ARDS patient on the “dry” side. In other words, avoid aggressive resuscitation with IV fluids. ARDS patients typically have increased WOB because the alveoli, lungs, and spaces between the alveoli are partially or completely fluid filled.
500
How do rns prevent ventilator acquired pna (VAP)?
good hand hygiene before & after sxn
wear gloves when providing oral hygiene
oral hygiene (Q2hrs)
sxn pt as needed for comfort
hob > 30-45 deg
turn per policy (Q2hrs)
early mobilization
spontaneous awakening trials per policy
daily spontaneous breathing trials
table 67.8 or table 32.8
500
BP 72/50, CVP= 24 (high), increasing oxygenation needs
a. nitrate
b. fluids
c. ionotrope/constrictor
d. diuretics
c. ionotrope/constrictor
Tank is full, need ionotrope/constrictor for increased cardiac contraction strength or vasoconstriction to help increase bp
500
Treatment modalities for the management of cardiogenic shock include (select all that apply)
a. vasoactive medications to improve myocardial contractility.
b. vasopressors to decrease systemic vascular resistance.
c. circulatory assist devices such as an intraaortic balloon pump.
d. corticosteroids to stabilize the cell wall in the infarcted myocardium.
e. Trendelenburg positioning to facilitate venous return and increase preload.
a. vasoactive medications to improve myocardial contractility
c. circulatory assist devices such as an intraaortic balloon pump: decrease afterload and L ventricular workload
Cardiogenic shock occurs when either systolic or diastolic dysfunction of the heart’s pumping action results in reduced cardiac output (CO), stroke volume (SV), and BP.
Specific measures to restore myocardial blood flow include angioplasty with stenting, emergency revascularization, and valve replacement.
choice b = Vasopressors will increase in SVR by causing vasoconstriction. The increased SVR increases the workload of the heart and myocardial O2 demand. It can harm a patient in cardiogenic shock by causing further myocardial damage and increasing the risk for dysrhythmias. Use of vasopressor drugs is limited to patients who do not respond to fluid resuscitation. Adequate fluid resuscitation must be achieved before starting vasopressors because the vasoconstrictor effects in patients with low blood volume will cause further reduction in tissue perfusion. Typically, if the patient has persistent hypotension after adequate fluid resuscitation, a vasopressor (e.g., norepinephrine, dopamine) and/or an inotrope (e.g., dobutamine) is given.
choice d = corticosteroids decrease inflammation; increases capillary permeability to increase bp & increase hr
choice e = preload is usually high in these pts without Trendelenburg positioning
preload= high
co= low
afterload= high
Pt will have increased hr and decreased bp; increased SVR will increase the workload on the heart - which will increase myocardial O2 consumption = low MAP; increased RR and crackles on auscultation; peripheral hypoperfusion; decreased UOP; anxiety, confusion, agitation from impaired cerebral confusion
table 66.8 or table 42.8
500
A pt has the following mixed deep partial thickness and full thickness burn injuries: face, anterior neck, right anterior trunk, and anterior surfaces of the right arm and lower leg. (fig. 24.4 or fig. 26.4)
a. According to the Lund-Browder chart, what is the extent of the pt burns? ___ % total body surface area
b. According to the rule of nines chart, what is the extent of the pt burns? ___ % total body surface area
c. Is it possible to determine the actual extent and depth of burn injury during the emergent phase of the burn? Why or why not?
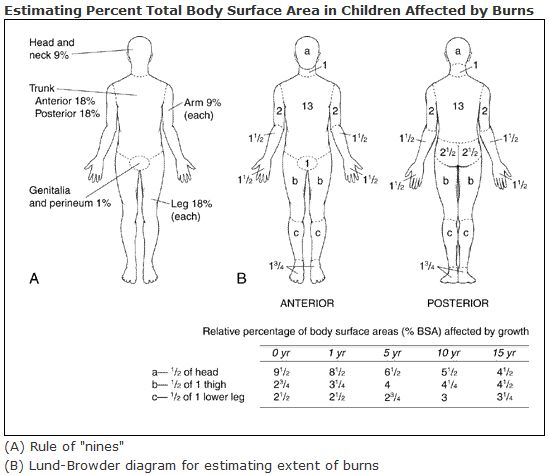
(fig. 24.4 or fig. 26.4)
a. Lund-Browder: 3.5 + 1 + 6.5 + 2 + 1.5 + 3.5 = 18% total body surface area
b. Rule of nines: 4.5 + 9 + 4.5 + 4.5 = 22.5% total body surface area
c. No, because edema and inflammation obscure the demarcation of zones of injury.
The emergent (resuscitative) phase is the time needed to resolve the immediate, life-threatening problems resulting from the burn injury. This phase usually lasts up to 72 hours from the time the burn occurred.
The main concerns are the onset of hypovolemic shock and edema formation.
The emergent phase ends when fluid mobilization and diuresis begin.