Ultrasound
ED Special Delivery
Resuscitation
Is My Discharge Abnormal
Bleeding
100
33 yo severe abdominal pain after a syncopal episode. VS BP 90/50 HR 122 O2 100% RR 18 afebrile. You start a fast exam and see the following:
What is the most likely diagnosis?
Ruptured Ectopic Pregnancy
100
30 yo G8P7 presents in active labor at approx 41 weeks. On your exam, baby is crowning but you notice the head is bobbing in and out. What is the diagnosis and what is your next move?
Shoulder dystocia
McRoberts Maneuver (hyper flexion at the hips) and suprapubic pressure
100
During CPR in the setting of pregnancy, what patient positioning maneuvers should be taken to optimize circulation?
Left lateral uterine displacement
100
A 25 yo F presents with malodorous grey/whote vaginal discharge. Under the microscope you see clue cells. What is the treatment?
Bacterial Vaginosis
Metronidazole PO or intravaginally
100
A 65 yo F presents with vaginal bleeding. She has been post menopausal for 10 years. What is the most likely diagnosis?
Cancer- endometrial (uterine)
200
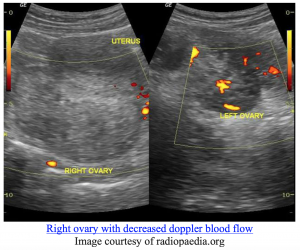 25 yo F with sudden onset severe RLQ pain. TVUS shows the above. What is the diagnosis and next step in management?
25 yo F with sudden onset severe RLQ pain. TVUS shows the above. What is the diagnosis and next step in management?
Ovarian Torsion. Consult OBGYN
200
30 yo G8P7 presents in active full term labor. On your exam, you see a prolapsed pulsating cord. What is the next step in management?
Elevate presenting fetal part, call OBGYN asap, patient will require emergency c section
200
What are symptoms of magnesium toxicity if given for preeclampsia/eclampisa?
Decreased respiratory drive, loss of reflexes, muscle paralysis
200
A 25 yo F presents to the ED with complaints of yellow/green vaginal discharge. On pelvic exam you notice a strawberry red cervix. What would you see under microscopic evaluation of discharge?
Motile flagellated cells
Trichomoniasis. Tx Metronidazole
200
A 24 yo F in 3rd trimester of pregnancy presents with severe abdominal pain after high mechanism MVC. You plate fetal parts on abdominal exam. What is the diagnosis?
Uterine rupture
300
27 yo F presents with history of prior pelvic inflammatory disease with new onset lower abdominal pain, fever, and vaginal discharge. Pelvic exam is notable for a unilateral tender adnexal mass. What is the diagnosis?
TOA
300
What is the most common cause of postpartum bleeding?
Uterine atony
300
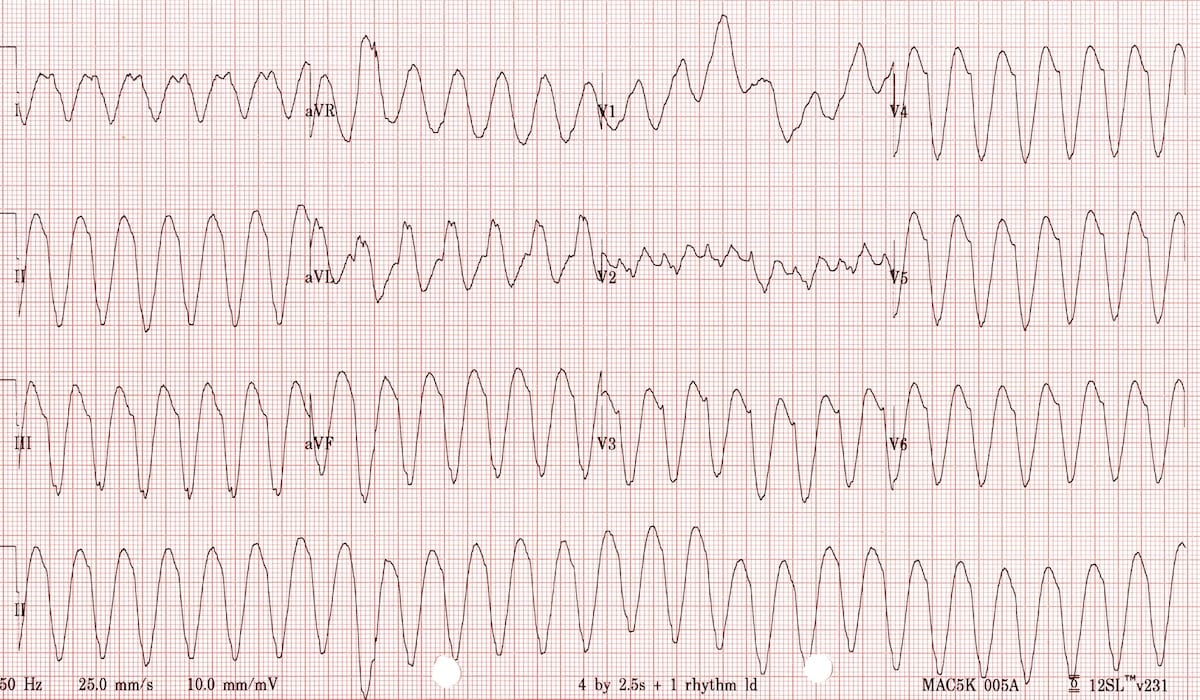 33 yo F 24 week gestation presents with palpations, CP and SOB. HR 165 BP 80/40 O2 99%. What is the next step in management
33 yo F 24 week gestation presents with palpations, CP and SOB. HR 165 BP 80/40 O2 99%. What is the next step in management
Cardioversion! Versed seems to be an acceptable option for sedation
300
33 yo F is requesting empiric treatment for STIs after exposure. What medications should be given?
Ceftriaxone 500 mg IM
Doxycycline 100 mg BID 7 days
300
What is the dose of rhogam in a spontaneous first trimester pregnancy loss in an Rh- negative patient?
50 mg IM
400
What is the beta-hcg discretionary zone for a visible intrauterine gestational sac with transvaginal ultrasound?
1500
400
30 yo G8P7 presents in active full term labor. You deliver the baby successfully, however, the patient continues to bleed. What is the dose and route of Pitocin that you can give in the emergency department quickly while waiting on drip from pharmacy?
10mg IM
400
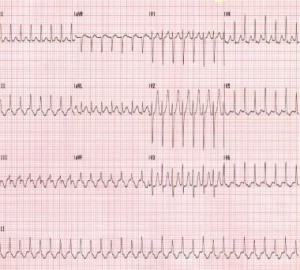 32 yo F approx 32 weeks gestation presents with palpitations. HR 150 otherwise VSS. Treatment?
32 yo F approx 32 weeks gestation presents with palpitations. HR 150 otherwise VSS. Treatment?
1. Vagal manuevers
2. Adenosine 6mg -> 12mg (safe in pregnancy, short acting, does not cross placenta)
400
33 yo F in 2nd trimester of pregnancy is requesting empiric treatment for STIs after exposure. What medications should be given?
Ceftriaxone 500 mg IM
Azithromycin 1g PO once
400
What presents with painless bright red vaginal bleeding in 24 week gestation pregnant woman?
Placenta previa
500
What three structures must be visualized to accurately measure bi parietal diameter?
Falx, cavum setpum pellucidum, and thalamus.

500
What are ways to tamponade uterine bleeding in a post part hemorrhage?
Bakri balloon
Foley catheter (may need more than one)
Pack with gauze
500
What is the dose of magnesium IV and IM for eclampsia?
IV 6mg bolus (15-20 min) and 2mg infusion/hour
IM 10mg (5mg/buttock) and 5mg e every 4 hours
500
What bacteria are the most common cause of PID?
Gonorrhea and chlaymdia
500
What are risk factors for Placental Abruption?
HTN
Cocaine
Cigarette Smoking
Multiparty
Trauma