Main Ideas
Main Ideas
Definitions
Definitions
100
Describe the anatomy and flow of blood through the 4 chambers of the heart.
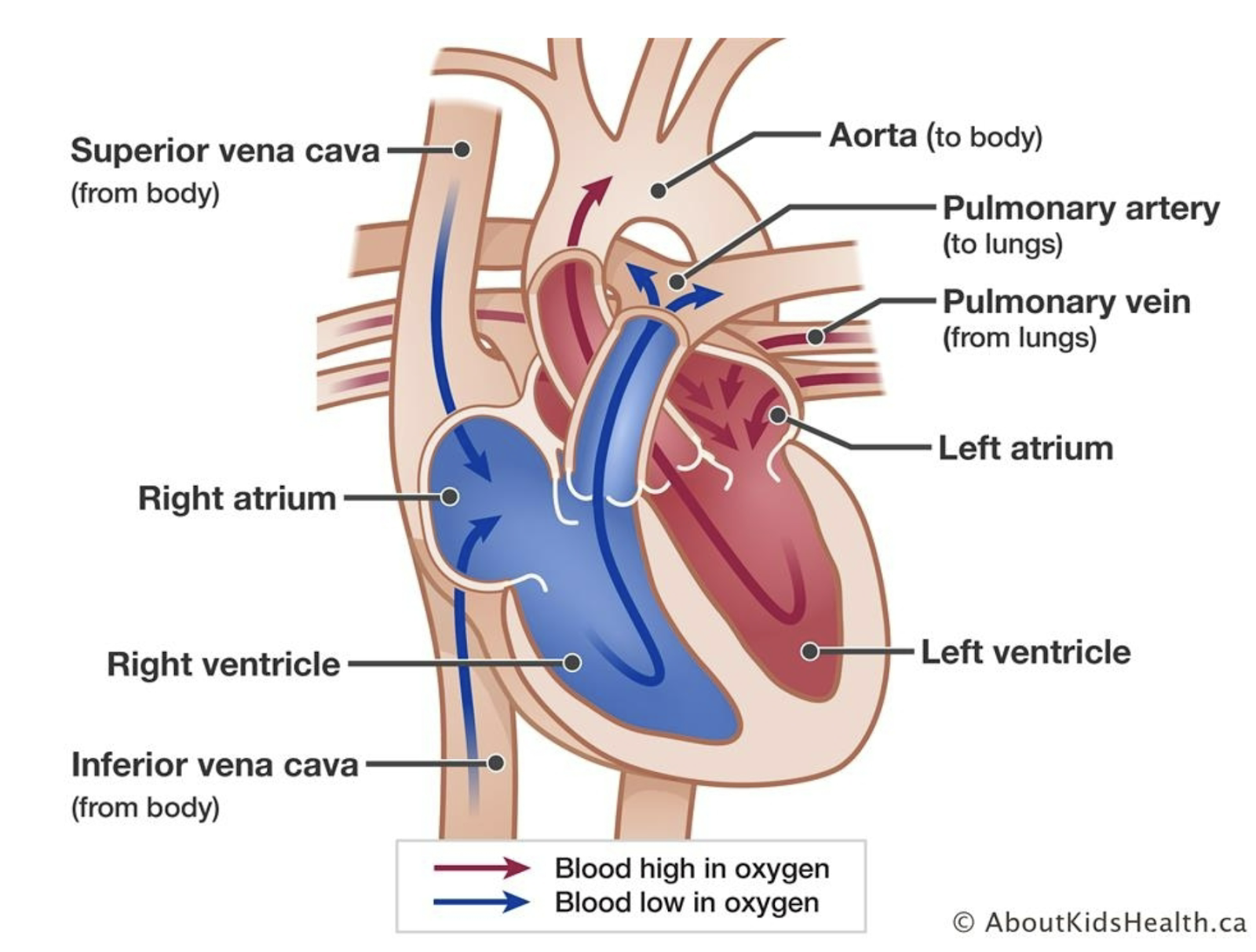
Blood low in O2 flows >Sup/Inf vena cava> Right atrium>Tricuspid valve>Right ventricle>Pulmonary artery>Lungs>Blood rich in O2 flows >Pulmonary vein> left atrium>Bicuspid valve> left ventricle> Aorta> Body
100
How to treat rhythmic arrhythmia
Treatments
Cardioversion: normal rhythm returns spontaneously (AF)
Defibrillator: electrical method (VF)
Pacemaker: implants designed to replace the heartbeat (heart block)
100
Causes of cardiac related chest pain
Ischemia, MI, pericarditis, endocarditis, aortic dissection
100
Disturbance of heart rate (normal 60-100 x/minute)
Tachycardia - >100 bpm
Increased sympathetic stimulation
Bradycardia - <60 bpm
Normal in well-trained athletes
Rate Arrhythmia
200
Common signs and symptoms of cardiac pathologies.
Chest, neck, arm pain/discomfort
Palpitations
Dyspnea
Cardiac syncope
Vasovagal syncope
- Cough
- Cyanosis
200
Explain how DVT and pulmonary embolism is formed
Formation: DVT typically occurs when a blood clot forms in a deep vein, often in the legs. These veins are responsible for returning deoxygenated blood back to the heart.
200
Irregular, fast or ‘extra’ heart beat
Occur with arrhythmias/dysrhythmias
Associated symptoms
Light-headedness, syncope
Can be benign
Caffeine, anxiety, exercise
Severe condition
CAD, cardiomyopathy, complete heart block, ventricular aneurysm
Palpitations
200
variations from the normal rhythm
Dangerous as they reduce cardiac output - perfusion of the brain and myocardium can be impaired
Ventricular fibrillation: non-coordinated muscular contractions of ventricular muscle
Heart block: irregular rate caused by an interruption in the passage of impulses through the heart’s electrical system; treated with medication and pacemakers
Atrial fibrillation: blood remains in the atria after they contract and ventricles do not fill properly; prone to blood clots
Rhythmic Arrhythmia
300
Describe the effects of aging on the CV system
Reduction in Function
Development of cardiac fibrosis
Reduction in calcium transport across membranes
Lower capillary density
Decreased adrenaline response
Impaired autonomic reflex control of heart rate (BP and HR control)
Fit and healthy adults, the heart will:
Pump less blood to the skin
Work harder under the same circumstances
Disease may have greater impact than CV function than aging
Heart disease begins earlier than formerly expected
Early findings in adolescents of cholesterol deposits in vessels
Cardiovascular disease
Most common cause of hospitalization and death in the older population
Effects of aging have less relevance at rest but considerable consequences during cardiac events
300
Medical management of a DVT
Primary prevention
Early mobilization
Prophylactic use of anticoagulants
Elastic stockings
Pneumatic pressure devices (mimic calf pump)
Ambulation after adequate anticoagulation therapy has been administered if symptoms and condition permit
300
Shortness of breath (SOB)
Can be cardiovascular, pulmonary, or due to trauma, fever, medications, or obesity
Dyspnea on exertion (DOE): dyspnea with mild exertion
Orthopnea - breathlessness which occurs with recumbency - relieved with sitting upright
Can occur day or night
Dyspnea
300
partial or complete occlusion of a vein by a thrombus (clot)
Inflammatory reaction in the wall of the vein
Common complication after surgical procedures or CVA
Clinical manifestation of DVT may take up to 4 weeks
May be asymptomatic; dull ache, tight feeling, pain in calf
Venous thrombosis
400
List the common causes of angina pectoris
chest pain or discomfort occurring when heart muscle does not get enough oxygen
Can start behind the sternum
May be mistaken for indigestion
Can feel tight and can radiate
400
Describe how orthostatic hypotension occurs
Orthostatic hypotension: significant drop in blood pressure when standing from sitting or laying down
Normal response - standing results in force of gravity causing venous pooling lower limbs
Compensatory mechanisms: increased HR, increased vascular resistance
Orthostatic hypotension - the body cannot compensate, loss of cerebral blood flow which may result in fainting
During supine → standing transition
Drop of >20 mmHg in systolic BP
Drop of >10 mmHg in diastolic BP
May see HR increase as well
Causes
Aging
Postural reflexes are slowed
Cardiac output decreases
Vasoactive HTN drugs
400
Fainting (mild form = light-headedness)
Reduced O2 to the brain when the heart’s pumping ability is compromised
Causes
Arrhythmias, orthostatic hypotension, aortic dissection, CAD
Cardiac syncope
400
embolus has traveled via the venous system into the heart then travels into a pulmonary artery and occludes it
Pulmonary embolism
500
Describe the types of angina pectoris
Stable angina
Exertional - predictable levels of physical or emotional stress and responds promptly to rest or nitroglycerin
No pain at rest
Location, duration, intensity, and frequency of chest pain are consistent over time
Unstable angina
Preinfarction angina
Unpredictable and not relieved by rest
Post-infarction angina
After MI when residual ischemia triggers an episode
500
Describe the different types of aortic aneurysms and where they occur
Aneurysms: abnormal stretching in the wall of vessel or chamber
Types:
Thoracic aortic aneurysm - above the diaphragm
Abdominal aortic aneurysm - below the diaphragm
May be asymptomatic initially then results in:
Persistent vague, substernal, back and neck pain
Rupture - tearing of the vessel walls with bleeding into the thoracic or abdominal cavity
May be identified by palpation of imaging
Medical screening questions are critical
500
Very strong parasympathetic response that leads to vasodilation throughout the body
As a response to emotional distress, heart rate slows and vessels dilate leading to hypotension and cerebral hypoperfusion = fainting
Vasovagal syncope
500
intermittent episodes of small artery constriction to the extremities
Causes temporary pallor and cyanosis of the digits and changes in skin temperature
Cold temperature
Strong emotion
Raynaud’s disease
600
Management of angina
Short acting sublingual nitroglycerine
Vasodilators: beta blockers
Calcium channel blockers: limit heart rate and contraction of heart
600
BP regulated by 2 factors
Blood flow (determined by cardiac output) and peripheral vascular resistance (diameter of vessels)
600
Usually associated with pulmonary conditions
Can be pulmonary complication of a cardiovascular condition
Left ventricular dysfunction with resulting pulmonary edema presenting as cough with aggravated by exercise
Dry and hacking
Hemoptysis: productive, frothy, blood tinged sputum with pulmonary edema
Cough
600
Narrowing that prevents the valve from opening fully; chamber behind the narrow valve must work harder
Stenosis
700
List common gender differences in the CV system
Coronary Artery Disease: leading cause of death and a significant cause of morbidity among women in the US
Women and minorities were underrepresented in studies conducted on heart disease
In general, patients with smaller bodies and smaller arteries have a higher mortality rate after CABG
Women may have CAD and microvessel disease - just opening the artery may not be sufficient
Coronary microvascular dysfunction
Tiny blood vessels to the heart become constricted - reducing blood flow
“Stealth” heart disease
May not show up on classic angiograms
Classic signs of reduced blood flow may not be present
700
_____ pressure: when heart contracts
_____ pressure: when heart is relaxed
Systolic
Diastolic
700
Bluish discoloration of the lips, nail beds, fingers, toes
Inadequate blood oxygen levels
Cyanosis
700
Regurgitation; valve does not close properly
Valve insufficiency
800
Explain the condition of Ischemic heart disease
AKA: Coronary Artery Disease (CAD) - coronary arteries carry O2 blood to the myocardium; one of the arteries become narrowed or blocked, areas of the heart muscle supplied by that artery do not receive sufficient O2 and become ischemic/injured = infarction may result
Modifiable Risk Factors
Cigarette smoke (leading cause)
Tobacco products (increase HR and BP)
Elevated cholesterol levels
Hypertension
Obesity (heart has to work harder)
Physical inactivity
Impaired glucose metabolism
Psychological factors and emotional stress
Moderate alcohol consumption
Non-Modifiable Risk Factors
Increasing age
Gender
Family history
Ethnicity
Social determinants of health
800
What is the most common site of a Myocardial infarction and why?
Most common site = left ventricle (chamber of the heart with the greatest workload)
800
Hallmark of right ventricular failure
Usually bilateral and dependent
Jugular venous distention
Abdominal distension - ascites
Peripheral edema
800
A significant drop in blood pressure when standing from sitting or laying down
Orthostatic hypotension
900
Medical Management of Ischemic heart disease
Prevention is the ultimate goal
Begins slowly in adolescence and develops slowly
Controlling cholesterol before atherosclerosis (thickening and hardening of arteries) has a chance to do damage
Exercise and physical activity
Moderate intensity for 30 mins on most days of the week
Independent of weight loss - significant beneficial effects on risk factors
One intervention with the ability to influence the greatest number of risk factors
Surgery
Angioplasty: open an occluded artery without opening the chest using inflated balloon
CABG: taking a portion of a vessel from the chest or leg and grafting it on the coronary artery
Coronary stents: stent in place to maintain an open vessel
900
Compensated CHF: combined efforts of the 3 mechanisms achieve a normal level of cardiac output
First: failing heart attempts to maintain normal output of blood by enlarging to hold a greater volume of blood
Short term improvement
Contractility muscle decreases
Second: Nervous system increases the stimulation of cardiac muscle
Increase in pumping, mass, strength
Hypertrophy leads to increased need for O2
Third: Kidney compensation
Water retention = increase blood volume, exacerbates edema
Expanded blood volume increases the load on an already compromised heart
900
Cramping or leg pain
Brought about by consistent amount of exercise or activity
Result of peripheral vascular disease
Most functionally debilitating of symptoms
Claudication (leg pain)
900
open an occluded artery without opening the chest using inflated balloon
Angioplasty
1000
Explain the pathophysiology and treatment of hypertension (HTN)
BP is the force exerted against the wall of the arteries
Systolic pressure: when heart contracts
Diastolic pressure: when heart is relaxed
Normal: <120 and <80
Elevated: 120-129 and <80
High: 130-139 or 80-89
High stage 1: >140 or >90
Crisis: >180 and/or >120
BP regulated by 2 factors
Blood flow (determined by cardiac output) and peripheral vascular resistance (diameter of vessels)
Prolonged HTN - elastic tissue is replaced by fibrous tissue; thickened artery wall has greater resistance to flow of blood
Prevention
Annual BP check
Physical activity/exercise
Weight control
Limitations on salt and alcohol intake
1000
Chest pain or discomfort occurring when heart muscle does not get enough oxygen
Angina pectoris
1000
taking a portion of a vessel from the chest or leg and grafting it on the coronary artery
CABG
1100
Explain what occurs in a myocardial infarction
Myocardium receives blood from 2 large coronary arteries and their branches
1 or more of these vessels may become occluded
Most common site = left ventricle (chamber of the heart with the greatest workload)
Common cause: clot of the anterior descending branch of the left coronary artery
Zone of infarction: cells die where they have been deprived of O2
Zone of injury: area surrounding infarction, less damage, may return to normal
Caused by ischemic and injured myocardial tissues
1100
coronary arteries carry O2 blood to the myocardium; one of the arteries become narrowed or blocked, areas of the heart muscle supplied by that artery do not receive sufficient O2 and become ischemic/injured = infarction may result
Ischemic heart disease
AKA: Coronary Artery Disease (CAD)
1100
______ - >100 bpm
Increased sympathetic stimulation
______ - <60 bpm
Normal in well-trained athletes
Tachycardia
Bradycardia
1200
Clinical manifestations of a myocardial infarction (MI)
Sudden sensation of pressure (crushing chest pain - can radiate to the arm, throat, neck and back)
Pallor
SOB
Profuse perspiration
Mid-thoracic pain
Abdominal pain and nausea
In women:
Chronic unexplained fatigue
SOB - sometimes in the middle of the night
1200
Persistent elevation of systolic BP >130mmHg, diastolic BP >80mmHg (or both) measured on 2 separate occasions
Hypertension
1300
Explain the symptoms of congestive heart failure (CHF)
CHF Compensatory mechanisms
First: failing heart attempts to maintain normal output of blood by enlarging to hold a greater volume of blood
Short term improvement
Contractility muscle decreases
Second: Nervous system increases the stimulation of cardiac muscle
Increase in pumping, mass, strength
Hypertrophy leads to increased need for O2
Third: Kidney compensation
Water retention = increase blood volume, exacerbates edema
Expanded blood volume increases the load on an already compromised heart
Compensated CHF: combined efforts of the 3 mechanisms achieve a normal level of cardiac output
Decompensated CHF: mechanisms are no longer effective and the disease progresses to the final stages of impaired heart function
Can range from mild to life-threatening fluid overload
Symptoms usually develop gradually so many people do not recognize or report the symptoms
1300
Development of ischemia with resultant necrosis of myocardial tissue
Any prolonged obstruction depriving the heart muscle of O2 can cause MI
Risk factors are same as CAD
Occur more frequently in the early morning hours
Myocardial infarction (MI)
1400
Medical management and exercise conditions of CHF
Medical management
Diet and exercise
Sodium restricted diet
Limited fluid intake
Pharmacotherapy:
Reduce hearts workload
Increase muscle strength and contraction
Decrease kidney compensation response
Medications
ACE inhibitors: increase renal blood flow and decrease vascular resistance - enhance diuresis
Diuretics: control fluid buildup
B-blockers: act on cardiac tissue to reduce contraction and rate
Exercise considerations
Monitor vital signs before, during, and after exercise
Monitor for decreasing BP
Monitor for dyspnea - aerobic capacity is likely impaired
Low RPE - light to somewhat hard
Exertional dyspnea - should not exceed a rating of mild
American College of Sports Medicine
Moderate intensity
40-60% VO2 max
2-6 minute bouts
2 mins of rest
Gradually increase intensity and duration
Individual goals and expected outcomes in mind
Avoid exercise taking vasodilator medication
1400
condition in which the blood is unable to pump sufficient blood to supply the body’s needs; caused by inadequate pump performance; backup of blood into the pulmonary veins = pulmonary congestion
Left ventricular failure = CHF
Right ventricular failure = cor pulmonale
Common complication of ischemic and hypertensive heart disease
CHF may develop after an MI
Congestive heart failure (CHF)
1500
Explain the electroconductive pathway through the heart and how an arrhythmia occurs
Electroconductive pathway:
HR and rhythm is regulated by the SA node
Signal travels through the conduction system
Through walls of atria
Down to AV node
Walls of ventricles
1500
When heart is extensively damaged, cardiac enlargement occurs, heart cannot completely eject blood from the left ventricle
Cardiomyopathy