Differential Diagnosis
Workup
Manifestations
Management
Complications
100
35F with LLQ, RLQ abdominal pain and small-volume diarrhea for one year. Negative anti-tTG, anti-endomysial antibody, fecal calprotectin, ESR/CRP. Abdominal US and CTAP negative. Worsens after meals and improves with bowel movement or flatus.
Irritable Bowel Syndrome (D)
100
31F (sexually active) with 1 wk dysuria not responsive to nitrofurantoin. Now with new vaginal discharge. Which two organisms MUST be tested for?
Chlamydia trachomatis
Neisseria gonorrhea
100
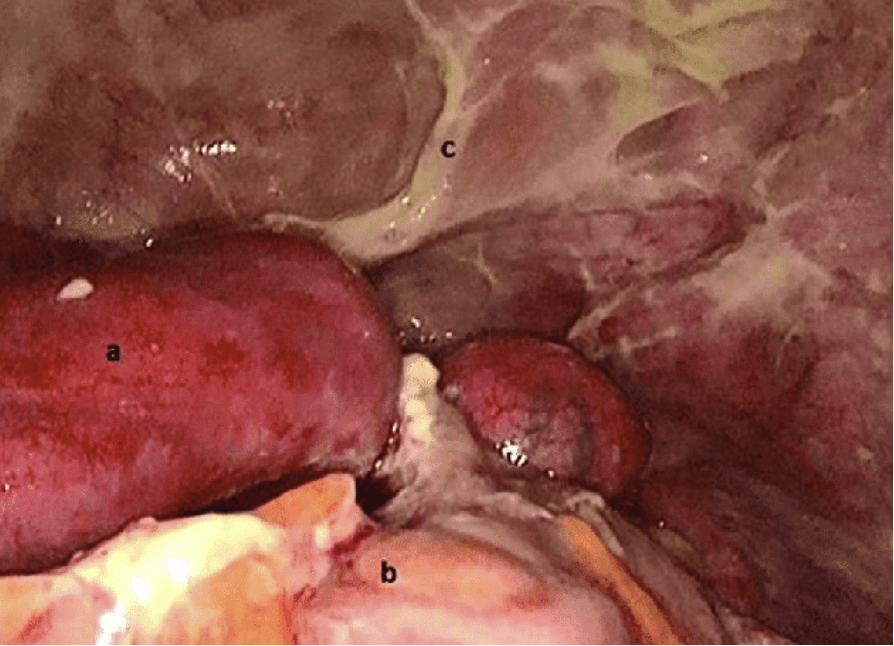
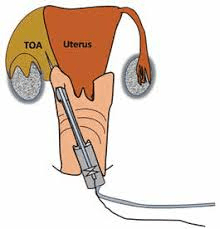
31F with L hemipelvic pain
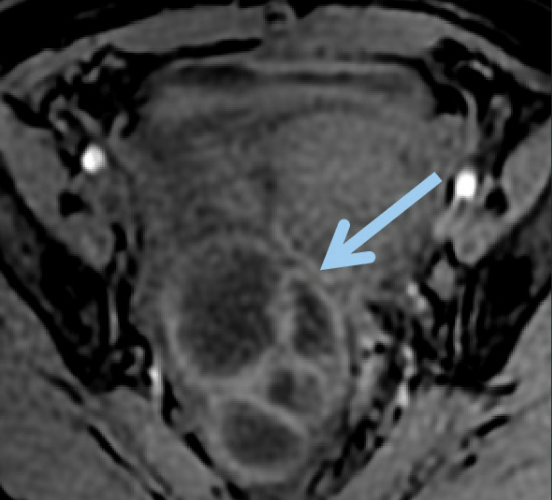
Tubo-Ovarian Abscess (TOA)
100
Two PO antibiotics are given as standard outpatient therapy for PID in a nonpregnant, nonlactating woman. One is Flagyl. Name the other.
Doxycycline 100 mg PO BID for 14 days
ALSO: Flagyl 500mg PO BID 14 days PLUS
Ceftriaxone 500 mg IM x 1 OR Cefoxitin 2 g IM x 1 AND Probenecid 1 g PO x 1
100
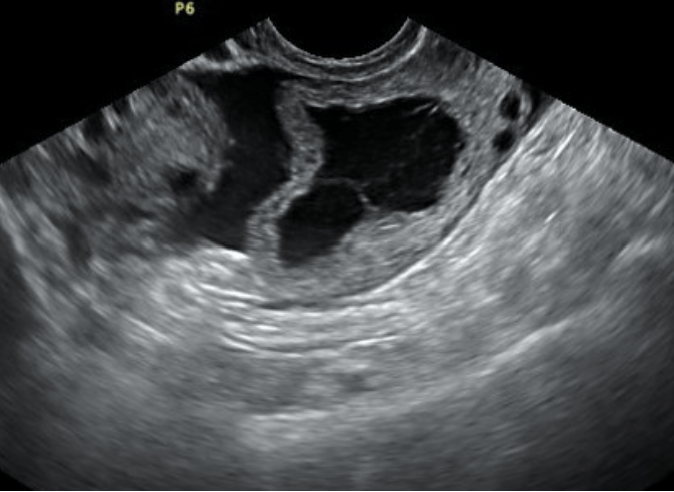
30F w/newly-discovered L TOA, now with rapidly-worsening L pelvic and groin pain:
Ovarian/adnexal torsion
200
26F with obesity, hirsutism, amenorrhea w/ one wk of worsening LLQ and pelvic pain not correlated w menses.
Ovarian cyst rupture
200
31F diagnosed with PID. Name three other screening labs that should be done.
HIV
Hepatitis B, C
Syphilis/RPR
Type-specific HSV serologies
200
31F with fevers and pelvic pain:

Endometritis/myometritis
200
The IV/IM version of this class of antibiotics is always added to PO regimens for PID.
Third-gen cephalosporins
Ceftriaxone
Ceftizoxime
Cefotaxime
200
24F with prior PID, now at 4 wks gestation w/ 2 days severe pelvic pain and vaginal spotting. b-HCG 5000.

Ectopic pregnancy
300
19F with months of lower abdominal and pelvic pain that becomes progressively more severe with menses and improves following menstruation. No abnormal bleeding or spotting. TVUS with small endometrial cyst.
Endometriosis
300
31F initially given PO Flagyl for foul-smelling vaginal discharge but did not finish; now returns with new pelvic/adnexal pain. Name either of two organisms that may have caused her PID.
Trichomonas spp
Gardnerella vaginalis (BV)

300
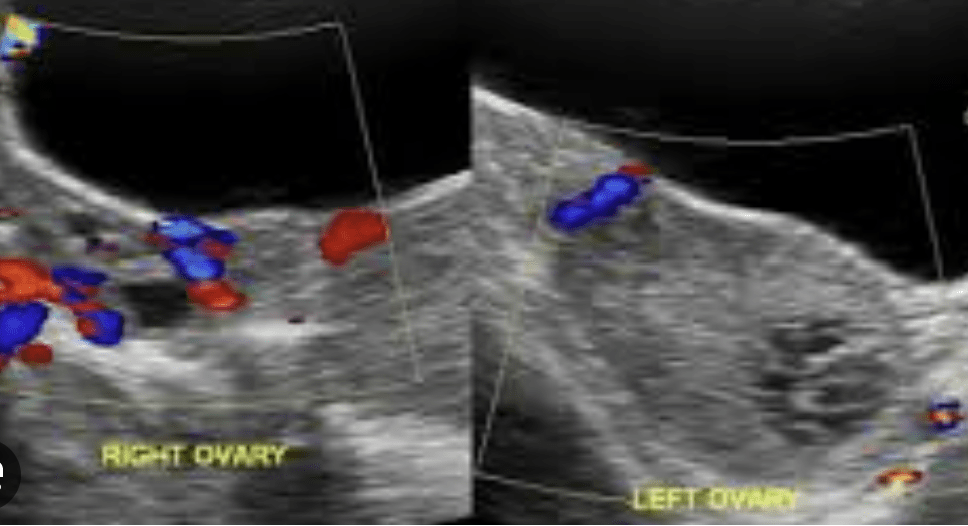
31F with L adnexal pain
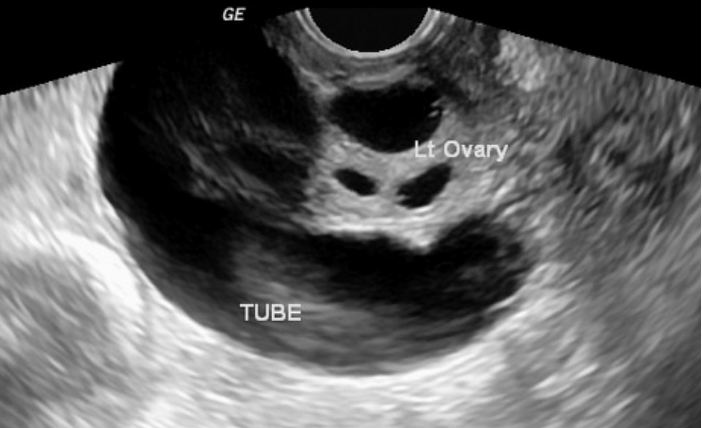
Salpingitis/hydrosalpinx
300
The CDC recommends 4 dual IV antibiotic combinations for inpatient treatment of (severe PID). Name one.
Cefotetan and doxycycline
Cefoxitin and doxycycline
Clindamycin and gentamicin
Ampicillin-sulbactam and doxycycline
300
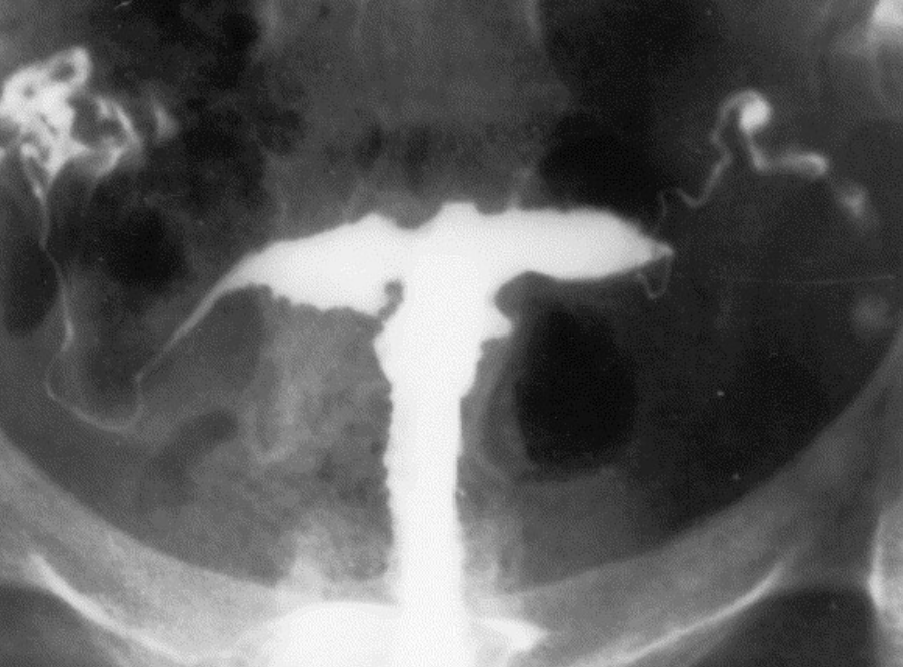
26F with prior PID with b/l TOA who cannot become pregnant despite multiple tries. Bloodwork negative. Partner's workup negative. What fluoro-based exam can serve as next step in workup?
Hysterosalpingram
400
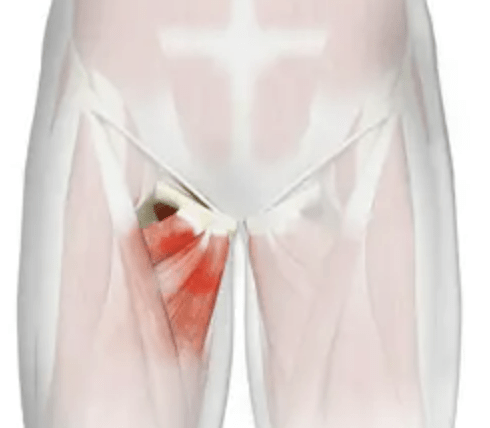
19F soccer player with several months of pelvic and groin pain, esp around inguinal ligaments. Pain increases when flexing trunk or hips.
Athletic pubalgia
400
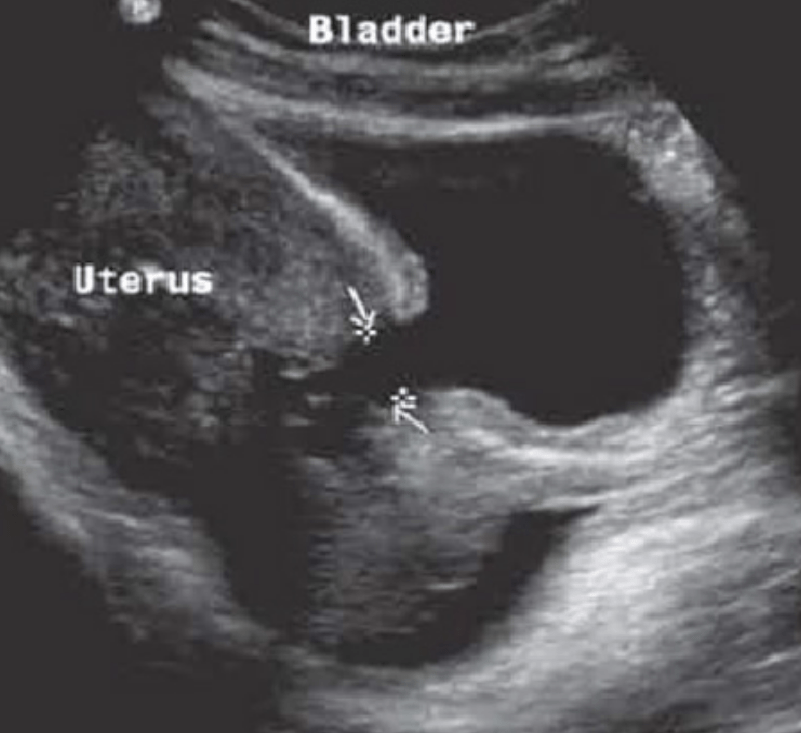
31F with suspected PID. What noninvasive imaging modality should be chosen for initial evaluation?
TVUS (Trans-Vaginal Ultrasound)
400
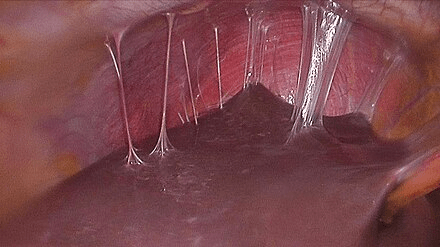
31F with active PID, also c/o vague RUQ pain and with newly-elevated LFTs.
Fitz-Hugh-Curtis Syndrome ("perihepatitis")
400
Name four criteria for hospitalization of a Patient with PID
- Cannot exclude surgical emergency
- Pregnant
- Abscess suspected
- Severe illness: N/V, high fever/instability
- Failure to respond to outpatient therapy.
- Cannot follow/tolerate outpatient therapy
400
34F with prior PID c/o a few yrs irregular menses (from every month to q3 mos and now q6 mos), hair under lip/chin, and hot flashes. Name three labs that can confirm this syndrome.
Premature/Secondary Menopause
Anti-mullerian hormone
Inhibin B
Estradiol
FSH/LH
500
36F with RA on MTX reporting three months of diffuse crampy abdominal pain, N/V, and weight loss. Has new job as social worker in a prison.
Tuberculous peritonitis
500
31F highly suspected to have PID, but with equivocal findings on multiple imaging studies (CT, TVUS, MRI). What diagnostic intervention should be pursued next?
Exploratory laparoscopy
500
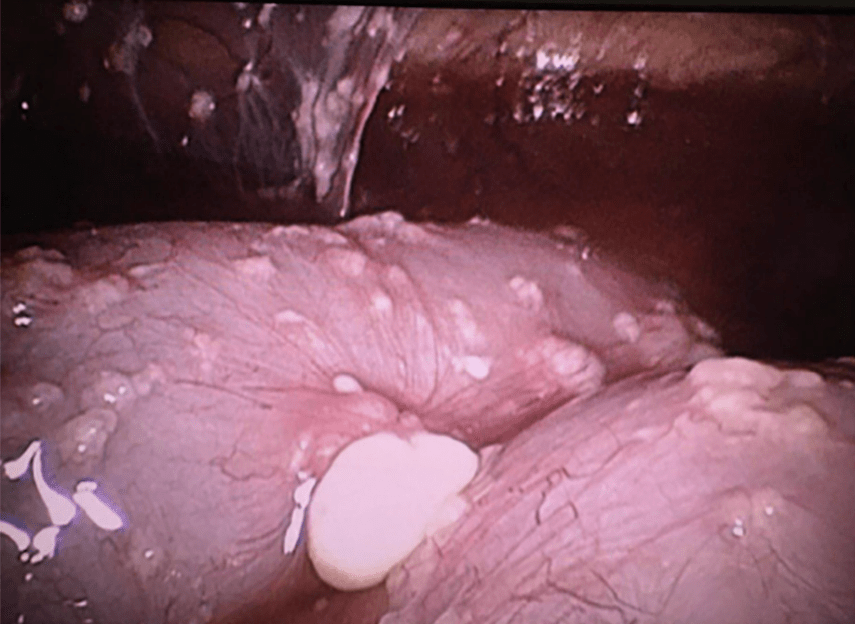
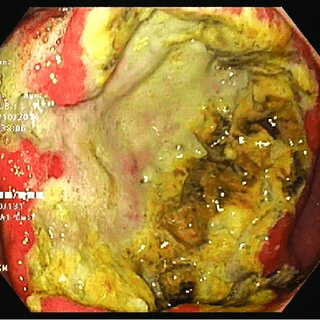
26F w/IUD (> 5 yrs overdue for replacement) c/o two months of pelvic pain, low back pain, and foul-smelling vaginal discharge with "yellowish-green specks".
Pelvic/IUD-associated Actinomyces
500
IR-guided drainage of TOA is becoming increasingly popular to avoid risks of surgical evacuation. Name the two most-used approaches.
Percutaneous
Transvaginal
500
35F with prior PID (endomyometritis) s/p surgical evacuation, now with new pelvic pain, urinary incontinence (esp with standing) and intermittent hematuria:
Uterovesical fistula