Pathophysiology of HL
Pathophysiology of NHL
Clinical Presentation
Diagnostic Testing
Treatment
100
What is the most common type of HL?
Nodular Sclerosis
Bonus Question: What lymph node(s) does Nodular Sclerosis HL present in first?
100
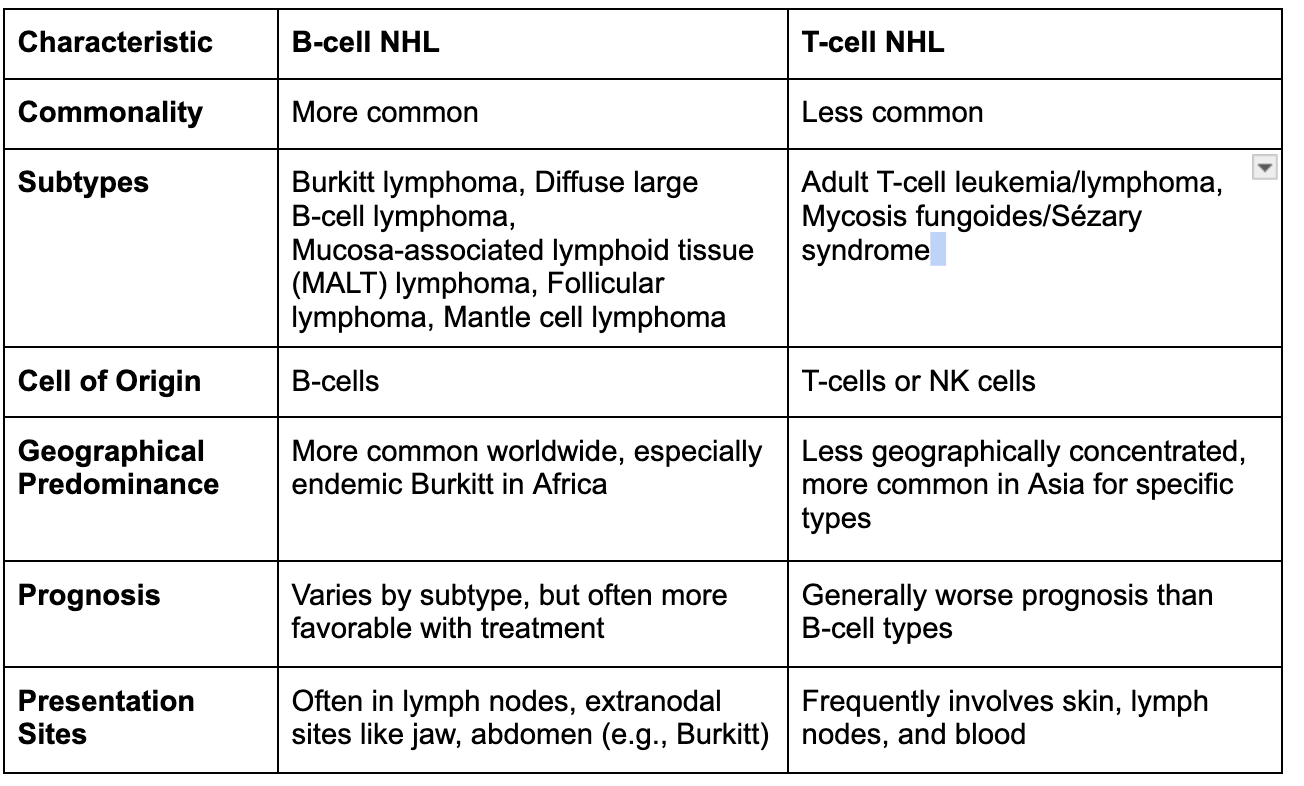
What are the two main types of lymphocytes involved in the pathophysiology of Non-Hodgkin’s Lymphoma (NHL)?
B-cells and T-cells
Bonus: Which type is more commonly affected in NHL?
Bonus: Differentiate between the key characteristics of B-cell and T-cell NHL.
100
A 25-year-old man presents with a painless, firm mass in his neck. He reports intermittent fevers, night sweats, and unintentional weight loss of 10 pounds over the last 2 months. A biopsy of the mass shows Reed-Sternberg cells. What is the most likely diagnosis?
Hodgkin Lymphoma
Bonus: What is the specific type of fever pattern seen in some patients with Hodgkin Lymphoma?
100
According to WHO, what is absolutely necessary for the definitive diagnosis for lymphoma?
Answer: Lymph node biopsy (or tissue biopsy depending on presentation of lymphoma)
100
Your patient is being treated for Acute lymphoblastic leukemia and would like to know how their chemotherapy is killing their cancer cells. What is the mechanism of action of Methotrexate?
Answer: Folate (B9) analog that inhibits the S phase of the cell cycle by inhibiting dihydrofolate reductase and therefore inhibiting DNA (thymidine) synthesis. This prevents DHF from being regenerated to THF to be used by thymidine synthesis in the conversion of dUMP to dTMP.
Bonus: A patient undergoing treatment with Methotrexate begins to complain of easy bruising, fatigue, and chills. What drug is indicated to resolve these symptoms?
200
What is the precursor to Reed-Steinberg cells?
B-lymphocytes (in germinal centers)
200
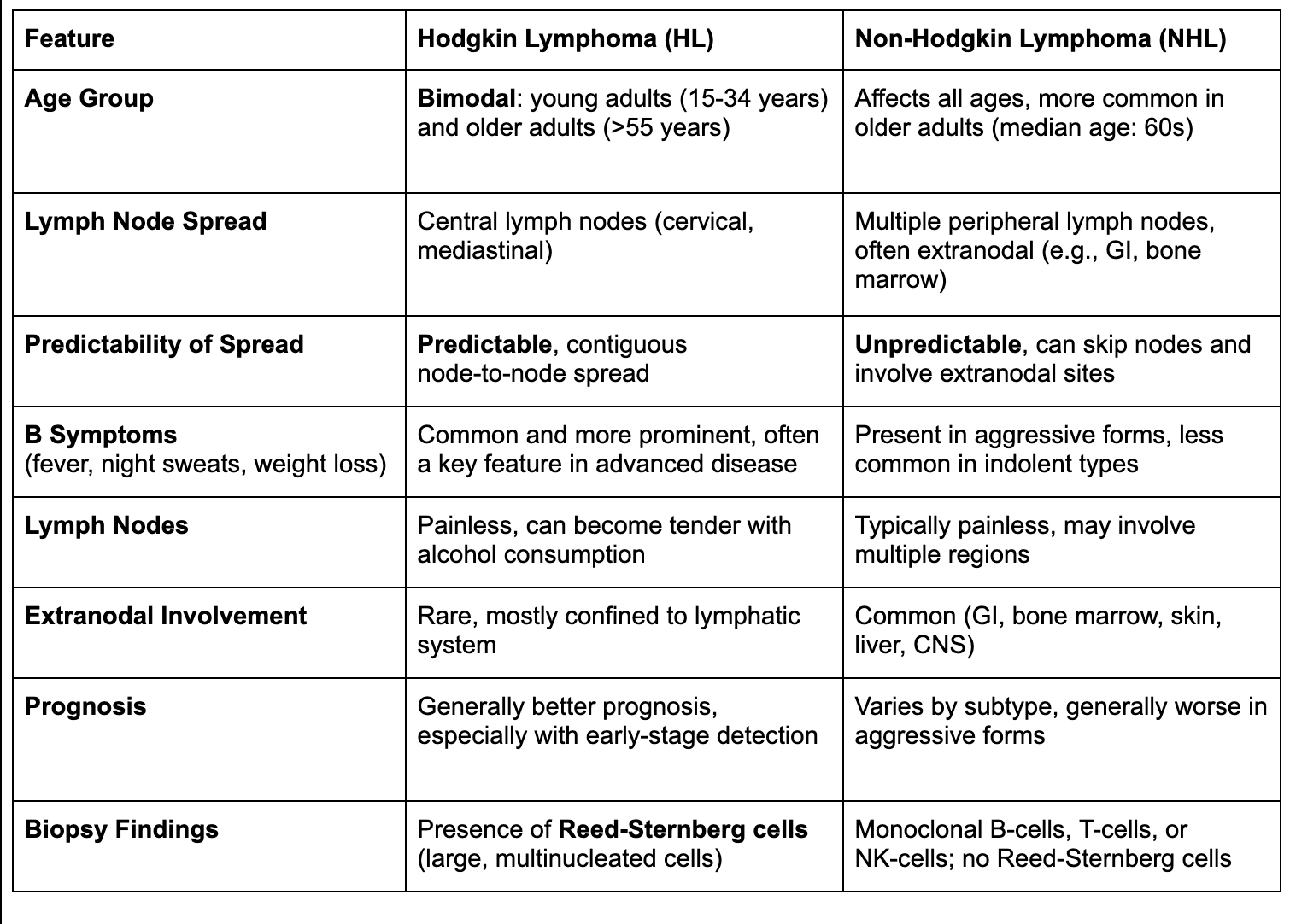
What contributes to the better prognosis of Hodgkin Lymphoma compared to Non-Hodgkin Lymphoma?
Due to its more predictable spread pattern, higher responsiveness to chemotherapy and radiation, and its tendency to be diagnosed at earlier stages. Additionally, Reed-Sternberg cells tend to be localized and easier to target with treatment. These cells are also more responsive to radiation and chemotherapy.
Bonus: How does the presence of B symptoms influence prognosis in both HL and NHL?
200
A 55-year-old woman presents with rapidly enlarging, painless lymph nodes in her groin and axilla, which developed over the past two weeks. She reports significant fatigue, occasional fever, and unintentional weight loss of 10 pounds in the last month. On examination, her lymph nodes are firm, mobile, and non-tender. Imaging reveals lymph node involvement in both the pelvis and mediastinum. A biopsy shows diffuse sheets of large, atypical B-cells. Based on these findings, what is the most likely diagnosis?
Diffuse Large B-cell Lymphoma
Bonus: What markers are expressed on malignant B-cells in Diffuse Large B-cell Lymphoma?
200
What does a high ESR indicate?
Answer: Inflammation in the red blood cells
Bonus question: How is the ESR measured? What is the difference between ESR & CRP?
200
You diagnose a patient with Acute Myelogenous Leukemia and plan to begin them on a chemotherapy regimen immediately. What is first line therapy for AML?
Answer: all-trans-retinoic acid (ATRA) (a form of vitamin A)
Bonus: What is the mechanism of action?
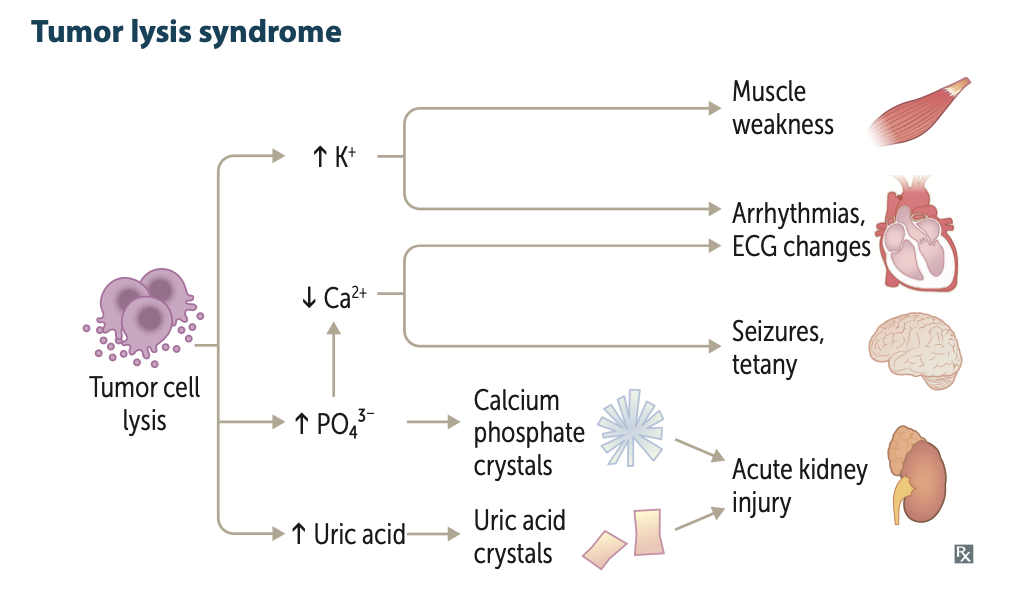
Bonus: Would the patient benefit from co-administration of Allopurinol?
300
Theorize - How does EBV lead to potential increase in Hodgkin’s Lymphoma?
EBV infects B-cells, leading to insertion of genome and proliferation/mutation in B-cells to proliferate RS cells
300
What role chromosomal translocations play in the development of certain subtypes of Non-Hodgkin’s Lymphoma (NHL)?
Chromosomal translocations in NHL can lead to the deregulation of oncogenes, promoting uncontrolled cell growth.
Bonus: Explain the significance of t(14;18) in follicular lymphoma.
Bonus: What chromosomal translocation is characteristic of Burkitt Lymphoma, and how does it affect cell proliferation?
300
A 25-year-old HIV-positive man presents with a 2-week history of rapidly enlarging, painless lymph nodes in the neck and groin. He also reports fevers and unintentional weight loss. Examination reveals firm, non-tender lymphadenopathy, and biopsy reveals a high-grade lymphoma with a "starry-sky" pattern. What is the most likely diagnosis, and what cytogenetic abnormality is characteristic of this disease?
Immunodeficiency-associated Burkitt Lymphoma, associated with t(8;14) translocation.
Bonus: Explain histology of "Starry-sky" appearance.
Bonus: What additional complication is this patient at risk for?
Bonus: Which genetic mutations, other than t(8;14), are associated with Burkitt lymphoma?
300
Point to both your left supraclavicular lymph node and right axillary lymph node.
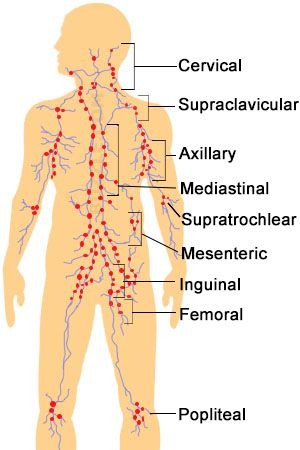
What is the supraclavicular lymph node in between? What about the axillary lymph node?
300
What is the mechanism of action of Cyclophosphamide and what is a potential long term outcome of this drug?
Answer: Alkylating agent that crosslinked DNA at guanine N7 and acts non-specifically on the cell-cycle. Alkylating agents have a high propensity for causing secondary malignancies such as Acute myelogenous leukemia (AML)
400
You are a pathologist assigned to read a cervical lymph node biopsy for a 62 year old male presenting with night sweats, unintentional weight loss and non-tender cervical lymphadenopathy. If the biopsy were to reveal a Hodgkin lymphoma, what would you expect to be the predominant cell type within the lymph node?
Answer: “reactive cells” (lymphocytes, plasma cells, neutrophils, eosinophils, and histiocytes) responding to Reed Sternberg cells. The composition of the reactive cells give rise to the clarifications of the HL subtypes. The Reed Sternberg cells make up the minority.
Bonus 1: What is the relationship between the Reed-Sternberg cells and the “reactive cells”?
Bonus 2: How does this relate to the patients presenting symptoms?
Bonus 3: What is a unique abnormal lab finding that can be indicative of Hodgkin Lymphoma?
400
What role does Epstein-Barr Virus (EBV) play in the pathogenesis of Burkitt lymphoma?
EBV drives B-cell proliferation and increases the likelihood of chromosomal translocations like the MYC translocation.
Bonus: What role does malaria play in the pathogenesis of Burkitt lymphoma?
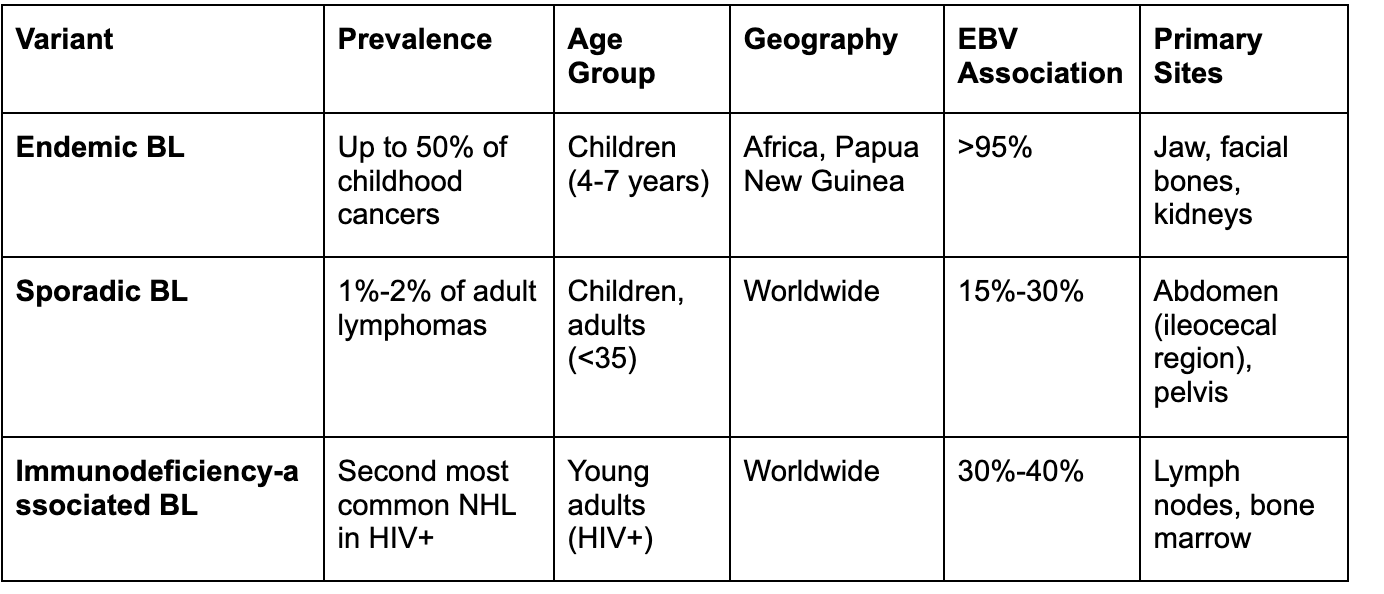
Bonus: What are the three clinical variants of Burkitt lymphoma based on the WHO classification?
400
A 30-year-old woman presents with a painless mass in her neck that she noticed about 3 months ago. She reports occasional chest discomfort and a persistent cough, but denies fever, weight loss, or night sweats. A chest X-ray reveals a mediastinal mass. A biopsy of the cervical lymph node shows lacunar cells and fibrosis, with a nodular pattern. What is the most likely diagnosis?
Nodular Sclerosis Hodgkin Lymphoma
Bonus: What is the prognosis for Nodular Sclerosis Hodgkin Lymphoma compared to other subtypes?
400
List the five types of Hodgkin’s Lymphomas and one histological characteristic that makes them unique from the other subtypes.
Classical
Nodular Sclerosis - fibrous bands, lacunar cells
Lymphocyte rich - Increase in mature lymphocytes, low amount of RS cells
Mixed cellularity - no fibrous bands, premature RS cells + inflammatory infiltrates
Lymphocyte depleted - low mature lymphocytes; high RS cells
Non-classical
Lymphocyte Predominant - No RS cells, but popcorn cells (giant, multilobed nucleus)
400
Name the 5 drugs used in ABVD treatment of Hodgkin Lymphoma and describe their mechanism of action.
- Doxorubicin Hydrochloride (Adriamycin) → free rad- DNA breaks; inhibits topoisomerase II
- Bleomycin—> free radical generation → DNA breaks
- Vinblastine Sulfate: Inhibits M phase of cell cycle → inhibits microtubule polymerization
- Dacarbazine: Cell cycle non-specific → alkylates DNA → crosslinks
500
A patient is undergoing a workup for suspected Hodgkin Lymphoma. Lymph node biopsy reveals Reed-Sternberg cells with surrounding reactive cells. If this patient is to have a good prognosis, would you expect to see a high or low concentration of lymphocytes?
Answer: The Lymphocyte rich subtype of HL is associated with an excellent prognosis as opposed to the Lymphocyte depleted subtype of HL. Therefore, we would expect to see an abundance of lymphocytes making up the majority of the reactive cells.
Bonus: why?
500
Describe the role of germinal centers in the development of B-cell Non-Hodgkin Lymphoma (NHL).
Germinal centers are areas within lymph nodes where B-cells mature and undergo processes like somatic hypermutation and class switching, which, if dysregulated, can lead to mutations and malignant transformation.
Bonus: What mechanisms allow malignant B-cells to escape immune detection in NHL?
500
A 55-year-old man presents with generalized pruritus and painless lymphadenopathy in the cervical and axillary regions. He reports recent episodes of fever and night sweats but has not experienced significant weight loss. A lymph node biopsy reveals a cellular infiltrate including eosinophils, plasma cells, and Reed-Sternberg cells. What is the most likely diagnosis?
Mixed Cellularity Hodgkin Lymphoma
Bonus: What imaging modality is most commonly used to stage HL, and what is it used to assess?
500
A 28-year-old female presents with a 3-month history of painless swelling in her neck and intermittent fever, night sweats, and weight loss.
Fast forward a week later, you have told the unfortunate news to the same patient that they have been diagnosed with Nodular Sclerosis Hodgkin’s Lymphoma. The good news is that you caught it early and it looks like a good prognosis. Walk through how you came to this definitive diagnosis, and what you ordered.
WBC with differential: Normal
ESR: elevated
LDH: elevated
CRP: elevated
PBS: RS Cells
Lymph node biopsy: Lacunar cells + fibrous bands
Flow Cytometry: CD15+, CD30+
500
You are an oncologist seeing a patient who is about to start ABVD chemotherapy. They are very nervous to begin treatment and are curious about the potential side effects of this treatment regimen. Sit the patient down and counsel them on the importance of receiving treatment and what side effects they can expect.
Common: high blood pressure, pancytopenia (infection, bruising, anemia), n/v/d, fevers, chills, muscle weakness, and fatigue
Infertility
High blood pressure which may cause headaches, dizziness, blurred vision
Infection, possibly in the blood, especially when white blood cell count is low
Anemia which may cause tiredness, or may require transfusion
Bruising, bleeding
Nausea, vomiting, loss of appetite, constipation
Sores in mouth or throat which may cause difficulty swallowing
Muscle weakness
Pain in the bones, jaw, and at the tumor
Fever, chills (occurring within 3-6 hours after administration)
Red colored urine, saliva, or sweat
Tiredness
Changes in skin or skin color, including darkening or thickening of skin, dark stripes on skin, skin rash or colored bumps on finger tips, palms, or elbows and toes, swelling of fingers, skin redness or tenderness, or itching
Hair loss