Neurology
Pharmacology
Misc1
Anxiety
Misc2
100
Which of the following was the most important factor in determining treatment outcomes in the National Institute of Mental Health (NIMH) Treatment of Depression Collaborative Research Program (1996)?
A.Interventions based on cognitive-behavioral therapy (CBT)
B. Psychopharmacological management
C. Interventions based on interpersonal therapy (IPT)
D. The therapeutic alliance
E. Placebo plus clinical management
The therapeutic alliance
No therapy is going to be very effective without the basics of warmth, empathy, and a therapeutic alliance.
100
Which of the following medications is FDA indicated for the treatment of GAD?
1. Imipramine
2. Paroxetine
3. Sertraline
4. Pregabalin
5. Bupropion
Paroxetine is the correct choice. Many SSRIs and serotonin-norepinephrine reuptake inhibitors (SNRIs) have effectively treated GAD in clinical trials, but paroxetine (Paxil), escitalopram (Lexapro), duloxetine (Cymbalta), and venlafaxine (Effexor) are approved by the U.S. Food and Drug Administration (FDA) for this indication.
100
A 5-year-old boy is brought to the clinic by his mother due to certain problems at school. The patient started going to school 2 months back and appeared to be doing fine. His teacher recently told his mother that the child persistently refuses to speak or answer any questions in the class since his arrival. The teacher thought that the child was adjusting to the new environment and did not inform the parents earlier. The mother states that the patient is very talkative at home and plays with his siblings and children in the park. He did not report any problems at school himself, saying it was "fine." The child is a bit shy but talks a lot when he gets to know people. He can tie his shoelaces, dress, and feed himself. He can count to 10 and can draw a square. Physical examination does not show any abnormalities. Which of the following is the most likely diagnosis in this patient?
A. Normal behavior
B. Adjustment disorder
C. Selective mutism
D. Separation anxiety
E. Stranger anxiety
The correct response is selective mutism as this patient refuses to speak in a specific social gathering (his school) where he is required to speak for at least one month. The child converses normally in places he feels comfortable (home, park) and has no other language or communication issues.
Normal behavior is incorrect as the refusal to talk in school can result in impairment of social and academic development of this child and should not be considered as a normal shy attitude in this case.
Adjustment disorder is incorrect as it is not diagnosed when symptoms meet the criteria for another disorder. This patient's refusal to speak in school for >1 month is consistent with selective mutism.
Separation anxiety is incorrect as it is characterized by extreme anxiety when separated from home and excessive worrying about losing close people. This patient does not refuse to go to school or cry, which excludes separation anxiety disorder as the likely diagnosis.
Stranger anxiety is incorrect as it is characterized by anxiety and distress on meeting new people, even in the presence of a familiar person. It is a normal finding in children 6-9 months of age and generally subsides by 3 years of age.
100
Childhood physical and sexual abuse has been shown to be a risk factor for which of the following anxiety disorders?
1. Specific phobia
2.OCD
3. Social phobia
4. GAD
5. Panic disorder
Panic disorder is the correct choice. There is a study from Stein that early life trauma or maltreatment is a risk factor for panic disorder,
100
A 33-year-old man is brought to the physician due to behavioral changes leading to suspension from his job. For the last 8 months, his mood has been unpredictable. Sometimes, he is anxious, irritable, and paranoid that his coworkers are conspiring against him, and at other times, he is quiet and withdrawn. He recently accused his staff of planting a microphone in his laptop and listening to everything that he says. His temperature is 99°F (37.2°C), blood pressure is 160/90 mm Hg, the pulse is 104/min, and respirations are 16/min. Physical examination reveals pupillary dilation, diaphoresis, and mild tremors. A mental state examination reveals an irritable, anxious man who is restless and hypervigilant during the entire examination. His speech is pressured and difficult to interrupt. Which of the following is the most likely cause of anxiety in this patient?
A. Delusional disorder
B. Paranoid personality disorder
C. Cocaine use disorder
D. Major depressive disorder
E. Phencyclidine intoxication
The correct response is cocaine use disorder as it is characterized by sympathetic stimulation leading to tachycardia, pupillary dilation, tremors, and diaphoresis. Psychiatric manifestations include anxiety, irritability, mood swings, and psychotic symptoms like paranoia and hallucinations. Its withdrawal results in depression and lethargy. This patient's anxiety and physical symptoms are best explained by this disorder.
Delusional disorder is incorrect as it is characterized by persistent delusions without any other psychotic symptoms for ≥1 month. This disorder cannot explain this patient's anxiety or physical findings.
Paranoid personality disorder is incorrect as it involves a lifelong pattern of pervasiveness and mistrust in individuals without any psychotic symptoms. It cannot explain this patient's irritability, anxiety, and physical symptoms.
Major depressive disorder is incorrect as it is characterized by depressed mood and/or anhedonia among other symptoms, for >2 weeks. Depression does not typically lead to the physical findings seen in this patient (dilated pupils, tachycardia, hypertension, diaphoresis and tremors). This patient's quiet and withdrawn behavior at times is likely due to cocaine use disorder.
Phencyclidine intoxication is incorrect as it is characterized by psychotic symptoms and aggressive behavior, including violence. It can present with anxiety and irritability, but the most prominent physical symptom, in this case, is nystagmus, which is not observed in this case.
200
Which of the following will be seen in patients on neuroimaging during tic suppression?
A. Increased activity in the frontal cortex
B. Increase activity in globus pallidus
C. Increase activity in the putamen
D. Decrease activity in the caudate nucleus
E. Increase activity in the thalamus
Tic suppression involves inhibition of unwanted impulses by the neural circuit that consists of prefrontal, parietal, temporal, and cingulate cortices associated with modulation of activity in the basal ganglia and thalamus. Excitatory projections from the prefrontal cortex synapse on the caudate nucleus which then sends inhibitory projections to globus pallidus and substantia nigra via GABAergic neurons. Fibers then project to thalamus from substantia nigra from where the neurons project back to the cortex. An increased activity in the frontal cortex is noted during tic suppression on neuroimaging. There is a decrease in the globus pallidus activity during tic suppression. There is a decrease in the activity of the putamen during tic suppression There is an increase in the activity of the caudate nucleus during tic suppression. There is decrease in the activity of thalamus during tic suppression.
200
A 29-year-old man presents to the clinician complaining of sleep disturbances, restlessness, and difficulty acquiring erections for the past 9 months. The patient has difficulty falling asleep and wakes up several times every night. The patient says that he worries about failing law school, paying his bills, and disappointing his parents. He is no longer able to concentrate in class and failed his last exam. The patient has no history of any previous illness. He is sexually active with his girlfriend. The patient has a history of drinking alcohol excessively during his early 20s but has limited his consumption for the past 3 years. He appears to be anxious on mental status exam. Vital signs are normal. The patient is oriented to person, time, and place. No abnormalities are seen on physical examination. In addition to psychotherapy, which of the given drugs is most appropriate for this patient?
A. Propranolol
B. Mirtazapine
C. Lithium
D. Buspirone
E. Doxepin
The patient fulfills the criteria for generalized anxiety disorder (GAD) given excessive anxiety for over 6 months, difficulty controlling the anxiety, concentration impairment, sleep disturbance, and restlessness. 1st line medications are selective serotonin reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors (SNRIs); however, buspirone is also FDA indicated for GAD treatment. Typically it is not as effective at treating symptoms of GAD as SSRIs and is used primarily as an augmentation agent. Still, it has a favorable side effect profile making it a good option for this patient given his sexual dysfunction. SSRIs are associated with decreased libido or erectile dysfunction.
Answer A is incorrect. Propranolol is incorrect since it is more appropriate for managing situational anxiety.
Answer B is incorrect. Mirtazapine is primarily used for treating major depressive disorder or insomnia and does not have an FDA indication for GAD.
Answer C is incorrect. Lithium is a mood stabilizer used with bipolar disorder and not for GAD.
Answer E is incorrect. Doxepin is a tricyclic antidepressant that is no longer considered a first-line option for treating generalized anxiety disorder due to more potential side effects but may be an option to help with insomnia.
200
A 23-year old man is brought to the clinic by his brother because of restlessness and lack of sleep at night. He was diagnosed with schizophrenia 2 months ago and started on appropriate therapy. His brother says that 2 weeks after starting therapy, the patient developed difficulty walking and a tremor that improves with activity. He says that the tremor keeps the patient up at night. The temperature is 98.1°F (36.7°C), pulse is 90/min, respirations are 20/min, and blood pressure is 120/86 mm Hg. Which of the following is the most likely cause of this patient's latest symptoms?
A. Cholinesterase inhibitor
B. Gamma-aminobutyric acid agonist
C. Dopamine agonist
D. Dopamine antagonist
E. Acetylcholine antagonist
D. Dopamine antagonist
Explanation:
Dopamine antagonist is correct because dopamine 2 receptor antagonism is the main mechanism of action for antipsychotics, especially first-generation antipsychotics such as haloperidol. All antipsychotics that interact with the D2 receptor can cause extrapyramidal syndrome, but this effect is particularly pronounced in the use of first-generation antipsychotics due to their high affinity to D2 receptors. Patients who have taken antipsychotics for weeks can show Parkinsonism, including tremors, rigidity, and shuffling gait, which this patient is experiencing.
Cholinesterase inhibitor is incorrect because it is the mechanism of action for medications that treat mild to moderate cases of Alzheimer's dementia and vascular dementia. Cholinesterase inhibitors, such as donepezil, increase the concentration of acetylcholine due to reduced degradation. Considering the lack of memory dysfunction in this patient, cholinesterase inhibitors would not have been indicated, nor would they have typically caused extrapyramidal symptoms (EPS).
Gamma-aminobutyric acid agonist is incorrect because direct GABA receptor agonists, such as barbiturates, and indirect GABA agonists like benzodiazepines, inhibit neuronal excitability and are used as sedatives. Either drug group does not typically cause EPS.
Dopamine agonist is incorrect because dopamine agonists, such as ropinirole, may be used in the treatment of Parkinson disease (especially earlier disease). This class of medication should not be given to patients with schizophrenia since they can further increase psychotic symptoms.
Acetylcholine antagonist is incorrect because central-acting anticholinergic agents like Atropine increases heart rate, reduces salivation, blurs vision, but does not typically induce EPS.
200
Psychiatric history does increase the risk for PTSD. Which psychiatric disorder most increases the risk for PTSD?
1. Depression
2. Bipolar disorder
3. Substance abuse
4. Somatization disorder
5. Generalized anxiety disorder
Depression - there appears to be strong evidence for depression increasing the risk of trauma and for developing PTSD, but the evidence for the risk of PTSD from substance abuse is equivocal. Certainly a depressed alcoholic would be at great risk for PTSD, but often it is the other way around. That is, usually affective, substance use, and somatoform disorders occur as a consequence of PTSD.
Comorbidity with mental disorders is common in PTSD. Epidemiologic samples have demonstrated that over 90% of people with PTSD have at least 1 lifetime comorbid mental disorder. Some of the most prevalent comorbid conditions with PTSD are major depressive disorder, alcohol abuse and (or) dependence, and another anxiety disorder. Self-medication of PTSD symptoms with alcohol and illicit drugs has been demonstrated to be associated with comorbid alcohol or drug use disorders. Among Axis II disorders, there has been increasing evidence that PTSD is associated with borderline personality disorder and antisocial personality disorder. It is possible that personality styles associated with impulsivity may put the person at risk of exposure to traumatic situations.
200
A 27-year-old woman with a history of paranoid schizophrenia presents to the clinic because of difficulty walking, feelings of restlessness and akathisia, and shaking movements of her hands that get worse when she lies down to sleep. Current medications include fluphenazine; her dose was recently increased. She is on a small dose of Lorazepam as well; but that dose has not changed. Which of the following choices would most likely improve her restlessness and be the safest clinical option?
A. Further increasing her fluphenazine
B. Removing her lorazepam
C. Adding propanolol
D. Changing her antipsychotic medication to clozapine
E. Switching from fluphenazine to haldol
Propanolol or Inderal may be beneficial for akathisia.
Choice A, this choice is incorrect because it is most likely the fluphenazine that has exacerbated or caused her EPS like complaints and akathisia.
Benzodiazepines have been seen as helpful in the treatment of akathisia, so removing her lorazepam would not help; actually, a small increase in the dose may help her complaints.
Clozapine is typically not associated with severe EPS or severe akathisia as would be seen in first-generation antipsychotics, but it has a serious side effect profile, including severe blood dyscrasias, that it is usually reserved for refractory cases of chronic psychosis.
Haldol is incorrect as it is not the most helpful option and is also a first-generation antipsychotic and strongly associated with EPS and akathisia.
300
A 15-year-old boy is brought by his parents, who are greatly distressed by their son's new behaviors. For the last week, he has been sleeping day and night, only waking to eat and use the bathroom. When he awakes, he is groggy and confused. His emotions are changed too. He appears apathetic, lethargic, and uncommunicative. The parents suspect drug use. Which one of the following conditions must be included in the patient's differential diagnosis?
A. Fragile X syndrome
B. Tuberous sclerosis
C. Major depressive disorder
D. Kleine-Levin syndrome
E. Cri-du-chat syndrome
Kleine-Levin syndrome is a rare neurological condition of unknown etiology that begins in childhood or adolescence and is characterized by episodes of hypersomnolence and altered behaviors during wakefulness. There is no definitive treatment, although stimulants are often prescribed to increase the period of wakefulness. Patients with Kleine-Levin syndrome are often misdiagnosed with a sleep, depressive, or substance use disorder. Fragile X syndrome is a genetic disorder with intellectual deficits. Patients typically have flat feet, large ears, a long face, and a prominent jaw and forehead. Tuberous sclerosis causes benign tumors throughout the body and seizures. There is no mention of depression or anhedonia, and the patient’s symptoms have only been present for 1 week, so it cannot be major depressive disorder. Cri-du-chat syndrome is caused by a deletion of part of chromosome 5, it results in a high-pitched cry and often results in death in the first year of life.
300
A 50-year-old man with a history of depression visits the ED after an episode of syncope. The patient says that he has had multiple episodic attacks consisting of palpitations and fainting. His medical workup including cardiac enzymes was unremarkable. The only abnormality was on ECG which was significant for a QTC of 612. Which of the following medications is most likely causing his symptoms?
A. Citalopram
B. Fluoxetine
C. Sertraline
D. Bupropion
E. Mirtazapine
Citalopram is the correct answer; it is a selective serotonin reuptake inhibitor (SSRI) that is recommended as the first line pharmacotherapy for the treatment of patients with major depressive disorder and is associated with QTc interval prolongation. This risk increases dramatically with doses over 40 mg daily. Answers B and C are incorrect. Fluoxetine and sertraline also are SSRIs, but do not prolong the QT like citalopram. Answer D is incorrect. Bupropion is a norepinephrine-dopamine reuptake inhibitor (NDRI) used for MDD. Notable side effects are increased risk of seizures (mostly seen in immediate release formulations), insomnia, and agitation. Mirtazapine is an atypical antidepressant used for depression and anxiety. Notable side effects are sedation and weight gain. Neither mirtazapine nor bupropion is associated with QTc prolongation at therapeutic doses.
300
A 23-year-old male patient with bipolar disorder is stabilized on lithium as inpatient. He does well over the next months as an outpatient with stable lithium levels. Then one hot June day he is brought to the emergency department with lithium toxicity. What is the most likely cause of this toxicity?
A. DehydrationB
B. Doubling of lithium dose
C. Low sodium diet
D.Starting an ACE inhibitor
E.Starting angiotensin II inhibitors
A. Dehydration
Explanation:
Lithium is a potent anti-manic agent used for the effective management of bipolar disorder as well as for unipolar depression. It does not bind to plasma proteins and is not metabolized. It is excreted through the kidneys so changes in the body's water and salt content can affect the amount of lithium excreted, resulting in either increased or decreased plasma lithium concentration. A decrease in body fluids resulting in dehydration leads to a build-up of lithium in the plasma which in turn results in lithium toxicity. There has been no indication to double the dose of lithium since the patient has been having steady plasma lithium levels, so this is not the cause of acute lithium intoxication. Low sodium diets can lead to potentially toxic concentrations of lithium, but in the given case, dehydration due to hot weather is the clear trigger. Starting an ACE inhibitor would cause initially decreased GFR but that would stabilize with time. Moreover, the history is not suggestive of any concurrent drug use.
300
A 30-year-old woman presents to the clinic with the complaints of dyspnea, dizziness, chest pain and palpitations. For the past two years she experiences these symptoms whenever she is exposed to insects. She gives the history of similar phobia in her mother. On examination, heart rate is 100 beats/min, and blood pressure of 120/80mmHg is recorded. ECG and chest x-ray are normal. She is offered multiple sessions of exposure therapy, but she refuses to take them due to her busy schedule and the high cost of the treatment. Which of the following is an appropriate treatment option for her?
A. Sertraline for 6-12 months
B. One-session exposure therapy
C. Quetiapine for 6 months
D. Sertraline for 3 months
E. Alprazolam for 3 months
This question describes a patient with specific phobia and one-session exposure therapy being the appropriate treatment for her as it is time saving and cost-effective. One-session exposure therapy is a type of massed exposure therapy used for the treatment of specific phobias. It combines exposure, cognitive challenges, participant modeling, and reinforcement in a single session, that takes a maximum of three hours. By this technique, the advantages of graduated exposure could be achieved in a one prolonged treatment session with good results. Some researchers say that one-session exposure may be slightly less efficient than multiple sessions, However, with this technique, patients show better compliance, and it is cost-effective as well.
Answer C is incorrect. Quetiapine is an antipsychotic and has no role in specific phobia alone.
Answers A and D are incorrect. Sertraline is a selective serotonin reuptake inhibitor class antidepressant and is not indicated in the treatment of specific phobias.
Answer E is incorrect. Alprazolam could ameliorate anxiety in the short-term, but in the long-term management of specific phobias, it has no role.
300
Which combination of medications has the best evidence for being an effective maintenance treatment to prevent relapse of major depressive disorder following a course of electroconvulsive therapy (ECT)?
A. Clomipramine and carbamazepine
B. Fluoxetine and bupropion
C. Fluoxetine and olanzapine
D. Nortriptyline and lithium
E.Sertraline and levothyroxine
An RCT conducted in 2001 and another conducted in 2007 showed that the combination of nortriptyline and lithium was superior to placebo and nortriptyline alone for the prevention of relapse of major depressive disorder after a course of ECT. An RCT conducted in 2006 showed that the combination of nortriptyline and lithium was as effective as maintenance ECT for the prevention of relapse of major depression following a course of ECT. A 2013 meta-analysis showed that the combination of nortriptyline and lithium and maintenance ECT were associated with very similar major depressive disorder relapse rates at 6 months after a course of ECT (37.7% vs 37.2%). Major depressive disorder relapse rates following ECT tend to be greater than 80% in placebo groups. The other medication combinations have not been found to be effective for this purpose.
400
A 20-year-old man is brought to urgent care clinic due to acute onset of headache, and pain surrounding his left eye. He has nasal stuffiness, rhinorrhea, and redness of the sclera of the left eye. He reports that a series of headaches have been going on for the past 4 weeks, with an average of 1 to 2 headaches per day. In addition to sumatriptan and steroids, which one of the following therapy approaches has been shown to be effective in the acute phase of this type of headache?
A. Acetaminophen and codeine
B. Hyperventilation
C. Oxygen
D. Botulinum toxin
E. No treatment is necessary because these headaches are benign
oxygen
This patient presents with cluster headaches. They may acutely be responsive to high-flow oxygen treatment (10 L/min via nasal canula or facemask for 10 to 15 minutes). Cluster headaches are the most common autonomic cephalgia and predominantly affect men. They are very severe headaches that typically occur every night for many days in a row, and can occur up to 8 times a day. Sumatriptan is a first-line medication, but intranasal dihydroergotamine, lidocaine or capsaicin maybe useful as acute abortive treatments. Prophylactic treatments include verapamil, lithium, steroids or anti-epileptics.
400
A 32-year-old man comes to the office with anxiety. He states that he gets really anxious while flying on an airplane and gets nausea, palpitations, shortness of breath, and trembling. He has always been afraid of flying, but it has recently become worse. It has happened 4 times in the last 7 months. He now tries to avoid flying altogether and travels by road mostly. When he has to fly for an important business meeting urgently, he gets very anxious about it and lies awake at night, thinking about it. Past medical history is not significant for any disorder. Physical examination is unremarkable, and his vitals are within normal limits. Mental state examination reveals an anxious and tense man. He says that he cannot follow-up with psychotherapy for now due to his busy schedule this month. Which of the following is the most appropriate medication for the acute management of this patient's condition?
A. Mirtazapine
B. Sertraline
C. Buspirone
D. Lorazepam
E. Venlafaxine
The correct response is lorazepam as it is a short-acting benzodiazepine that can be used acutely for the management of specific phobia when behavioral therapy is unavailable, as observed in this case. This patient's fear of flying, panic attacks, and avoidance behavior is characteristic of specific phobia. As the medication can be habit-forming it is best practice to give only a small number of pills.
Mirtazapine is incorrect as it is an antidepressant used in the management of the major depressive disorder. This patient's signs and symptoms are consistent with the diagnosis of specific phobia and not major depressive disorder.
Sertraline is incorrect as it is a selective serotonin reuptake inhibitor that is not used as a first-line medication for specific phobia as evident from this patient's symptoms, i.e., fear of a specific situation (flying) resulting in avoidance behavior.
Buspirone is incorrect as it is an anxiolytic used in the management of patients with a generalized anxiety disorder. This patient's anxiety is limited to a specific phobic stimulus.
Venlafaxine is incorrect as it is a serotonin-norepinephrine reuptake inhibitor that is not used as a first-line medication for specific phobia as evident from this patient's symptoms, i.e., fear of a specific situation (flying) resulting in avoidance behavior.
400
A 40-year-old woman presents to the clinic complaining of a lack of sleep, mainly due to a shaking motion of her hands. She says that whenever she sits or lies down, her hands start to shake. She also reports the slowing of body movements. Her slowed movements are most pronounced when she tries to get up. Her history is significant for schizophrenia and hypertension. She is unable to recall all of her current drugs. Her vital signs are normal. Which of the following is most likely to result in this patient's complaints?
A. Amitriptyline
B. Clozapine
C. Fluoxetine
D. Haloperidol
E. Tramadol
Haloperidol is correct because this patient has a history of schizophrenia and is complaining of movement bradykinesia and resting tremors. Haloperidol is an antipsychotic that is used for managing schizophrenia. It is known to result in extrapyramidal side-effects (EPS), which result in Parkinson-like symptoms.
Amitriptyline is incorrect because it is a tricyclic-antidepressant. TCA use is associated with anticholinergic (i.e., dry mouth, urinary retention, constipation, etc.) and antihistaminic (i.e., daytime somnolence) adverse effects. It is not known to result in extrapyramidal (EPS) related effects.
Clozapine is incorrect because it is a second-generation antipsychotic. It, too, is used for managing schizophrenia. However, unlike first-generation antipsychotics, (i.e., haloperidol, fluphenazine) it is less likely to result in EPS related effects.
Fluoxetine is incorrect because it is an SSRI that is used for managing depressive disorder. Common side-effects include diarrhea, SIADH, and sexual dysfunction.
Tramadol is incorrect because it is an opioid with some action at serotonin and norepinephrine reuptake receptors. Common side-effects include nauseas, itchiness, and constipation.
400
A 45-year-old man comes to the clinic seeking help to quit drinking alcohol. He mentions drinking around 10 glasses of alcohol a day, and how most of his time is spent drinking, getting alcohol or recovering from its effects. His heavy drinking started two years ago when he felt like he was constantly on edge and worrying about the smallest things for several months. He would be restless and fatigued and was having trouble sleeping. He started drinking more to keep his nervousness at bay, but now his drinking problem has resulted in problems at work as well as creating problems with this family. What is the most likely diagnosis?
A. Generalized anxiety disorder
B. Alcohol use disorder
C. Generalized anxiety disorder with comorbid alcohol use disorder
D. Panic disorder
E. Panic disorder with comorbid alcohol use disorder
Generalized anxiety disorder is characterized by excessive worry on most days for a period of at least six months. The patient is unable to control their worrying and experiences restlessness, easy fatigability, irritability, muscle tension, and sleep disturbances. It seems like the patient had been suffering from generalized anxiety disorder before he started drinking. Panic disorder is characterized by recurrent unexpected panic attacks with symptoms including palpitations, shortness of breath, dizziness, nausea, sweating, chest pain and fear of dying. The patient's history is not indicative of panic attacks, and hence panic disorder can be ruled out. Alcohol use disorder is characterized by a one year period of heavy drinking which has at least two of the following symptoms: alcohol consumption is more than intended, there have been unsuccessful attempts at cutting down on alcohol intake, a lot of time is spent obtaining, using or recovering from alcohol, continued use of alcohol in spite of recurrent interpersonal problems, failure to fulfill obligations at work, tolerance to alcohol and constant craving for alcohol. The patient meets the criteria for alcohol use disorder, however; the diagnosis cannot be made solely on the basis of alcohol consumption. The underlying cause must also be addressed. It is clear from the history that the patient has been self-medicating his anxiety through the use of alcohol. Hence the diagnosis will be generalized anxiety disorder with comorbid alcohol use disorder.
400
30-year-old woman is brought to the clinic by her mother. She complains of difficulty sleeping at night due to twitches of her face and an inability to concentrate throughout the day. The patient has been seeing a psychiatrist for over 5 years now. Physical exam shows repetitive facial grimaces with occasional protrusion of the tongue. The patient says that movement is not in her control. What is the mechanism of action of the drug most likely to be causing this patient's presentation?
A. Antagonism of noradrenergic and serotonin receptors
B. Antagonism of dopamine receptors
C. Inhibition of dopamine and norepinephrine reuptake
D. Inhibition of serotonin reuptake
E. Interaction with cation transport
B. Antagonism of dopamine receptors
Explanation:
Antagonism of dopamine receptors is correct because given that this patient has a greater than 5-year psychiatric history, it is likely she is suffering from a psychiatric disorder and is currently on medication (although it is not explicitly stated in the vignette). Anti-psychotics, especially first-generation antipsychotics are known for causing in movement-related adverse effects. This patient's out of control facial twitches and tongue protrusion is suggestive of tardive dyskinesia. It is an adverse effect that is associated with antipsychotic use at higher doses and longer durations, but can occur at any time. Antipsychotics work by blocking dopamine receptors.
Antagonism of noradrenergic and serotonin receptors is incorrect because this is the mode of action of mirtazapine. It is an antidepressant that is commonly associated with somnolence and weight gain.
Inhibition of dopamine and norepinephrine reuptake is the mechanism of action of bupropion. Bupropion can cause insomnia, decreased appetite and increase the risk of seizures, it is not associated with tardive dyskinesia.
Inhibition of serotonin reuptake is incorrect because this is the mode of action of selective serotonin reuptake inhibitors (SSRI). SSRIs are known to result in anxiety, insomnia, and nausea, and in rare cases, tremors.
Interaction with cation transport is incorrect because this is the mechanism of action of lithium. This drug is used as a mood-stabilizer, and it is known to result in hypothyroidism and nephrogenic diabetes insipidus.
500
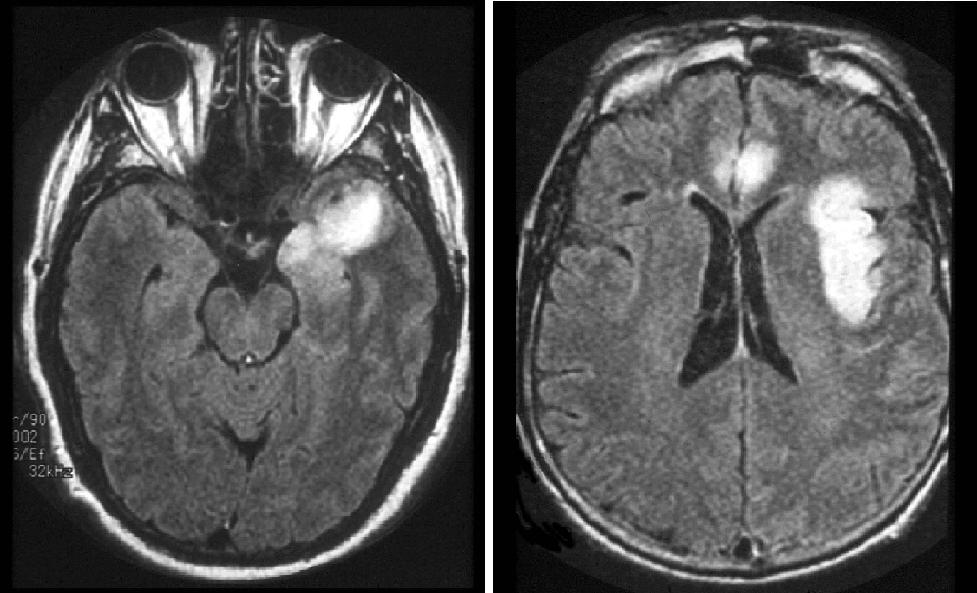
A 68-year-old previously healthy woman had 3 days of malaise and headache. For the last 24 hours, she seemed somewhat confused to the family and is brought to the ED because she was found sitting alone in the middle of the living room floor, mute. In the emergency department, she has a seizure and is comatose after. Her temperature is 39°C. No nuchal rigidity is present. Neurologic exam shows minimal response to deep pain. The right-sided extremities do not move and are more hyperreflexic than the left. There is a right Babinski sign present, and fundus exam shows no evidence of papilledema. Her MRI is shown. Which one of the following findings will most likely be shown on the patient's EEG?
A. Generalized 1 Hz periodic complexes
B. Periodic lateralizing epileptiform discharges (PLEDS)
C. Normal EEG patterns
D. Generalized spike-and-wave discharges
E. Nonspecific diffuse slow wave abnormality
Herpes simplex encephalitis typically presents with a several day history of fever and headache followed by memory loss, confusion, and seizures. The hallmark sign is a focal neurologic deficit suggestive of a structural lesion in the frontal-temporal areas. The EEG is often abnormal, demonstrating periodic sharp-wave complexes from one or both temporal regions on a background of low amplitude activity. PLEDS are often seen. On MRI images, the infection appears as regions of high signal intensity on T2 weighted images and fluid-attenuated inversion recovery (FLAIR) images. CSF should be sent for PCR assay for herpes simplex virus. Treatment is with intravenous acyclovir. PLEDs usually indicate an acute destructive cerebral lesion, generalized periodic sharp waves occur at a rate of 0.5 to 1 cycle per second. This pattern is commonly seen following cerebral anoxia and in 90 % of patients with CJD.
500
A 60-year-old man with bipolar disorder is diagnosed with hepatitis C. He has been taking valproate for mood stabilization for many years. How should his mood be managed now?
A. Increase dose of valproate
B. Decrease dose of valproate
C. Maintain same dose of valproate
D. Add carbamazepine with valproate
E. Switch to gabapentin and aripiprazole
E. Switch to gabapentin and aripiprazole
Explanation:
Gabapentin is a safer option as it rarely causes hepatotoxicity. However, it cannot be used alone. The addition of an atypical antipsychotic like aripiprazole can be a good option as it is not associated with severe liver injury and can be safely given to achieve mood stabilization.
Valproate has a high chance of bringing about hepatotoxicity and should be avoided in patients with liver disease. Increasing its dose could put the patient even more at risk.
Valproate has a high chance of bringing about hepatotoxicity and should be avoided in patients with liver disease. Decreasing the dose isn’t enough, the patient should be taken off the drug.
Valproate has a high chance of bringing about hepatotoxicity and should be avoided in patients with liver disease.
Valproate has a high chance of bringing about hepatotoxicity and should be avoided in patients with liver disease. Carbamazepine must also be used very carefully due to its liver metabolism.
500
A 26-year-old woman comes with the desire to get pregnant. She has been taking carbamazepine for 2 years for bipolar disorder. She wants to get pregnant in the next year. How should she be managed?
A. Continue at current dose for now and reduce dosage once pregnant
B. Taper off carbamazepine and switch to valproate
C. Folic acid supplements, switch to lamotrigine, taper off carbamazepine
D. Reduce dosage of carbamazepine and taper off before pregnancy
E. Stop carbamazepine immediately, folic acid supplementation
Lamotrigine is considered safe in pregnancy and is a good alternative if the patient responds well to it. Folic acid supplementation is important to prevent neural tube defects, especially in women who have been taking carbamazepine.
Carbamazepine is a class D drug and generally should not be given during pregnancy. It has been implicated in several congenital malformations, although some studies say that it does not pose a significant risk. However, it is advised that women on carbamazepine should be supplemented with folic acid 2 months prior to pregnancy. As this is a planned pregnancy, switching to a safer option and supplementation should be advised.
Valproate is a far more dangerous alternative and has been shown to cause teratogenicity and hemorrhagic syndrome in the neonate.
Simply tapering off carbamazepine leaves the patient at risk for worsening her mood disorder which can also pose a risk to the pregnancy.
Stopping carbamazepine can cause withdrawal and worsen the patient’s mental health.
500
A 27-year-old man diagnosed with panic disorder has been on benzodiazepine monotherapy for the past 2 years. He wants to discontinue medication as he feels much better now. Which of the following psychotherapies can be helpful in the discontinuation of medication in this patient?
A. Cognitive behavioral therapy
B. Eye movement desensitization and reprocessing
C. Panic-focused psychodynamic psychotherapy
D. Interpersonal psychotherapy
E. Supportive psychotherapy
Cognitive behavioral therapy (CBT) is the correct answer as it is not only recommended for the treatment of panic disorder but has also shown benefit in helping patients discontinue benzodiazepines. Studies have shown that using CBT during the tapering of benzodiazepines in individuals with panic disorder is more successful in the long-term when compared with supportive medical management when tapering benzodiazepines. Eye movement desensitization and reprocessing (EMDR) is incorrect as it is used as psychotherapy in individuals with posttraumatic stress disorder (PTSD) and has no role in the treatment of individuals with panic disorder. Interpersonal psychotherapy is incorrect as it is recommended for the treatment of individuals with major depressive disorder. Supportive therapy is incorrect as it is used to strengthen the defense mechanisms of the individual to a prior level of functioning and is not recommended for the treatment of the panic disorder. Panic-focused psychodynamic psychotherapy (PFPP) is incorrect because although it is recommended for the treatment for panic disorder, it has no role as psychotherapy in discontinuation of medications, especially benzodiazepines.
500
25-year-old woman is brought to the clinic by her husband because of worsening agitation and restlessness for the past 2 weeks. She was diagnosed with schizophrenia 2 months ago and started on fluphenazine a month ago which is adequately controlling her psychotic symptoms. Over the past 2 weeks she complains that she is unable to sleep or rest, even for a little while. She feels agitated, walks around for hours continuously, and is unable to sit still. Which of the following interventions is indicated 1st line for this patient?
A. Increasing the dose of fluphenazine
B. Decrease the dose of fluphenazine
C. Adding Valbenazine
D. Give an injection of diphenhydramine
E. Give benztropine by mouth
B. Decrease the dose of fluphenazine
Explanation:
This patient appears to be suffering from akathisia, which is a type of extrapyramidal symptom (EPS) consisting of restlessness. The ideal first treatment is to lower the dose of the antipsychotic, or change to another agent that is associated with lower incidence of akathisia if the patient's psychotic symptoms are well controlled. Another strategy is to add twice daily propranolol, but usually optimizing the antipsychotic is the first step. Answer A is incorrect. Increasing the dose will likely make the patient's akathisia worse Answer C is incorrect. Valbenazine is incorrect because it is a vesicular monoamine transporter 2 (VMAT2) inhibitor that is used for managing tardive dyskinesia. Patients with tardive dyskinesia complain of abnormal movement of the mouth and facial muscles. This patient has not developed tardive dyskinesia but has akathisia. Answer D and E are incorrect. Anticholinergic medications can be used for the treatment of akathisia however, decreasing the dose of the offending agent, switching to another agent, or using propranolol are all strategies that are favored.