What's your top differential?
History and physical aren't always enough
When self-hypnosis doesn't work
I have to order tests and interpret them too??
Sorry to do this to you (it's ECGs)
100
A 68-year-old male smoker reports that for the last six months, he has developed a cramping pain in his right calf every time he walks approximately two blocks. The pain is predictable and reproducible. If he stops and stands still for two to three minutes, the pain promptly disappears, allowing him to continue walking. Most likely diagnosis?
Intermittent claudication/chronic peripheral arterial occlusive disease
100
A 67-year-old male with a 40-pack-year smoking history presents for a routine physical. He is currently asymptomatic, and his blood pressure is well-controlled. You are considering screening him for an Abdominal Aortic Aneurysm (AAA) based on his risk factors. What is the appropriate next step?
Ultrasound
100
A 68-year-old female is diagnosed with Atrial Fibrillation after presenting with palpitations. She has a history of hypertension but no previous history of stroke or heart failure. Her current blood pressure is 135/85 mmHg. What is the appropriate treatment/intervention?
Oral anticoagulation
100
A 60-year-old female presents with sudden, "ripping" chest pain. Her blood pressure in the right arm is 185/100 mmHg, while the blood pressure in her left arm is 150/85 mmHg
A difference in systolic blood pressure of >20 mmHg between the arms is a significant finding that suggests a possible aortic dissection
100
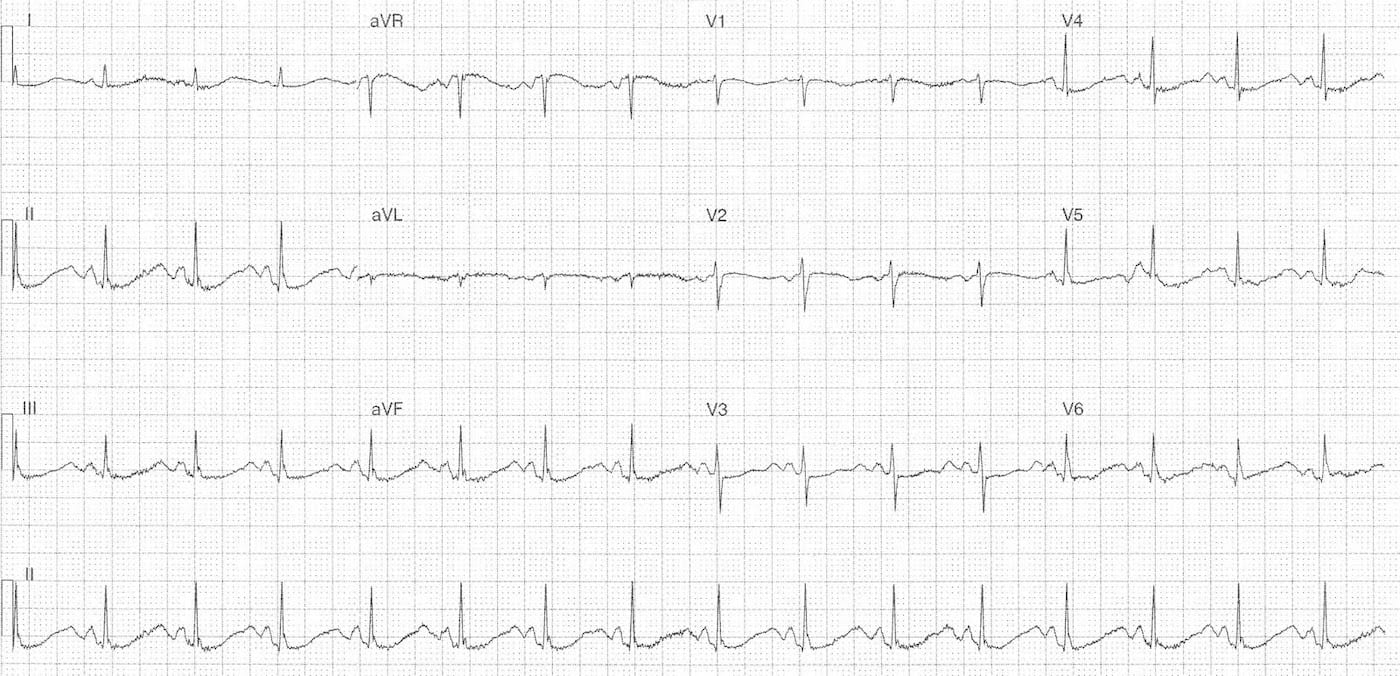
Diffuse ST segment elevations and PR depression (except aVR has PR elevation)
Pericarditis
200
A 72-year-old presents with progressive dyspnea on exertion and occasional syncope when walking uphill
On exam, harsh systolic murmur at the right upper sternal border that radiates to carotid. You hear an S4.
Most likely diagnosis?
Aortic stenosis
200
A 52-year-old patient with known hypertension presents with a blood pressure of 215/125 mmHg. They report a new, throbbing headache and blurred vision. You suspect a hypertensive emergency, which requires evidence of acute target organ damage (TOD). What is the appropriate next step?
Fundoscopy
200
A 45-year-old male is diagnosed with an Acute Stanford Type B Aortic Dissection. He is currently stable but has a heart rate of 95 bpm and a blood pressure of 165/95 mmHg. What is the appropriate treatment/intervention?
Beta blocker
200
A 65-year-old male undergoes a screening ultrasound of his abdomen, which reveals an infrarenal Abdominal Aortic Aneurysm (AAA) measuring 5.8 cm in diameter
Since the aneurysm is 5.5 cm, it has reached the threshold for surgical repair (open or EVAR)
200
Depressed ST segment, flattened T waves, prominent U waves and QT prolongation
Hypokalemia
300
A 62-year-old patient reports a "heavy" or "aching" sensation in the center of their chest that occurs whenever they walk up a steep flight of stairs. The sensation sometimes radiates to the inner left arm. The discomfort is predictable and disappears within 3 to 5 minutes once they sit down to rest. Most likely diagnosis?
Stable angina
300
A 60-year-old female presents to the Emergency Department with a sudden onset of "tearing" chest pain that radiates to her back between her shoulder blades. On examination, her blood pressure is 180/100 mmHg in her right arm and 150/85 mmHg in her left arm. What is the appropriate next step?
CTA
300
A 70-year-old male smoker with a history of Atrial Fibrillation presents with a sudden-onset cold, pale, and pulseless right leg. He has severe pain and some sensory loss in his toes (Rutherford Stage IIa). The contralateral limb has strong pulses. What is the appropriate treatment/intervention?
Embolectomy
300
Patient presents to hospital for 3rd CHF exacerbation, LVEF = 20%, cardiac index = 2 L/min/m2, and PCWP 30 mmHg. What stage of heart failure is this patient in?
NYHA III/IV (severe cardiac dysfunction)
300
ST depression, biphasic T waves in V1-V4 with reciprocal depression, and QT prolongation
Ischemia (likely in LAD)
400
A 19-year-old male athlete is brought in after a fainting spell during a high-intensity basketball game. His baseline ECG is unremarkable, but an exercise stress test is performed, which reveals bidirectional or polymorphic ventricular tachycardia triggered by the exertion. He has no known structural heart disease. Most likely diagnosis?
Catecholaminergic polymorphic ventricular tachycardia (CPVT)
400
A 55-year-old male presents with heavy, retrosternal chest pressure and diaphoresis that started 30 minutes ago. He looks pale and unwell. What is the appropriate next step?
ECG
400
A patient’s blood pressure remains uncontrolled despite being on an ACE inhibitor, a Calcium Channel Blocker (CCB), and a diuretic. What is the appropriate treatment/intervention?
MRA (spironolactone)
400
Patient presenting with general malaise has elevated WBC, positive rheumatoid factor, and elevated lactate. Suspected diagnosis?
Infective endocarditis
400
Wide QRS, RSR' pattern in V1-V3, wide slurred S waves in V5-V6
RBBB
500
A 28-year-old female presents to the emergency department with a sudden onset of "heart racing" that began while she was sitting at her desk. Her heart rate is regular at 180 beats per minute. An ECG shows a narrow QRS complex tachycardia, and P waves are not visible (they appear to be buried within the QRS complexes). Most likely diagnosis?
AVNRT
500
An 82-year-old male is brought to the clinic after a fainting spell that occurred while he was standing in line at the grocery store. He has a known history of heart disease. On physical examination, you hear a harsh systolic murmur at the right upper sternal border. What is the appropriate next step?
Transthoracic echocardiogram
500
Patient presents with altered mental status, cool extremities, BP 80/50, crescendo-decrescendo systolic murmur that radiates to neck. What is medication is indicated?
Vassopressor (norepi)
500
Patient presents with systolic crescendo murmur that gets louder with valsalva. ECG shows marked LVH. Most likely diagnosis?
HOCM
500
51 yr old female who presented with chronic vomiting. She has a history of rheumatoid arthritis and paroxysmal atrial fibrillation. What medication is contraindicated?
Digoxin