Got Gas?
Take My Breath Away
Vent Roulette
Guten Tag!
Fluid in the Wrong Places
Pop Caps
My Bad
Mad Skills
Picture This
100
This formula is used to calculate the anion gap.
Na⁺ − (HCO₃⁻ + Cl⁻)
100
The PaCO₂ threshold that defines Type II (hypercapnic) respiratory failure.
50 mmHg
100
These ventilator settings most directly affect oxygenation.
PEEP and FiO2
100
The Berlin Criteria attempts to exclude pulmonary edema secondary to this mechanism or mechanisms from its definition.
Cardiac failure or fluid overload
100
The best next diagnostic step for a new, unexplained pleural effusion on CXR.
Thoracentesis
100
The most common causative organism in community-acquired pneumonia.
Streptococcus pneumoniae
100
This is the amount of time since admission before a new pneumonia can be classified as hospital-acquired.
(Hint: It's the same threshhold for intubation and ventilator-acquired pneumonia.)
48 hours
100
These are two recognized complications of arterial line placement.
Arterial thrombosis and distal ischemia
100
No picture in this clue, but this modality is the cost-efficient initial radiologic exam for a patient presenting with cough, SOB, sputum production, and fever.
Chest X-ray
200
Septic shock, AKI, elevated lactate, and salicylate poisoning are all associated with this type of metabolic acidosis.
High anion gap metabolic acidosis
200
A patient with COPD exacerbation, cardiogenic pulmonary edema, or acute hypercapnic failure may benefit from NIV — but a patient with this neurologic finding would NOT.
Acute encephalopathy
200
This is a good starting volume target for your patients with and without ARDS.
6 ml/kg (IBW)
200
This is the most common indirect (extrapulmonary) cause of ARDS.
Sepsis
200
CHF, cirrhosis, and nephrotic syndrome all produce this type of pleural effusion through increased alveolar-capillary membrane permeability.
Transudative effusion
200
This is the appropriate antibiotic coverage for most patients with non-severe community-acquired pneumonia with no MRSA or pseudomonal risk factors.
- Typical organisms (beta lactam): ceftriaxone, ampicillin/sulbactam, cefotaxime
- Atypical coverage: azithromycin, clairithromycin, doxycycline
- Alternate monotherapy: levofloxacin, moxifloxacin
200
This is the typical recommended duration of antibiotic therapy for a patient with HAP or VAP.
7 days
200
The bedside test performed before arterial puncture to confirm adequate collateral circulation.
Allen test
200
The most rapid bedside tool for diagnosing pulmonary edema.
Bedside ultrasound (POCUS)
300
Watery diarrhea, renal tubular acidosis, and large-volume NS resuscitation share this common acid-base disturbance and its underlying mechanism.
Non-anion gap (hyperchloremic) metabolic acidosis from bicarbonate loss or dilution
300
This non-invasive mode of "ventilation" is ideal for patients with isolated hypoxia.
CPAP
300
This ventilator pressure reflects alveolar pressure and lung compliance.
Plateau pressure
300
The primary mechanism driving alveolar membrane injury in ARDS.
Pro-inflammatory cytokine cascade
300
Bacterial infection can cause this type of effusion
Exudative infection
300
In patients with established MRSA colonization or risk, one of these two drugs should be started.
Vancomycin or linezolid
300
These drugs reduce acid content in the oropharynx and might lead to colonization by nosocomial pathogens.
Proton pump inhibitors and H2 blockers
300
The most appropriate first step in preparing for endotracheal intubation with hypoxia.
Preoxygenation with 100% FiO₂
300
This finding on POCUS chest indicates what problem with the lungs.
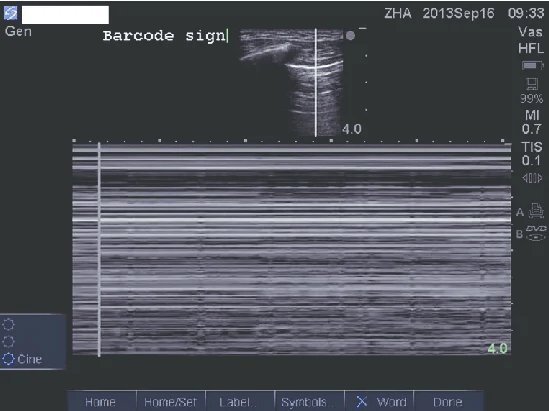
Absence of lung sliding
400
Calculating this value is useful in the presence of an anion gap metabolic acidosis.
Delta-delta anion gap
400
A patient with hypercapnic or mixed respiratory failure requires this mode of noninvasive ventilation.
BiPAP
400
These four types of alveolar injury result from ventilator mismanagement
Barotrauma, volutrauma, atelectrauma, and oxygen toxicity
400
Prone positioning is used to improve oxygenation in ARDS but does NOT reduce the risk of this ventilator complication.
Ventilator-associated pneumonia (VAP)
400
After determining an effusion is exudative, these three further tests are indicated on the pleural fluid.
Pleural fluid glucose, cytology, and culture
400
This intervention may reduce mortality in severe CAP.
Low-dose corticosteroids
400
For a patient with recent MRSA history being admitted for CAP, this screening test helps guide whether MRSA coverage should continue.
MRSA nasal screening
400
A cuff leak test is performed before extubation primarily to assess risk of this complication.
Post-extubation stridor (laryngeal edema)
400
Name this finding on chest X-ray.
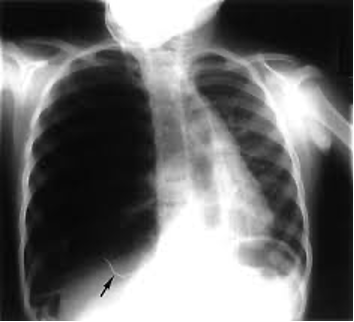
Tension pneumothorax
500
Though not specified in the typical anion gap calculation, this element of the comprehensive metabolic panel makes an outsized contribution to the anion gap.
Albumin
(corrected AG = measured anion gap x 2.5 (4-albumin))
500
The legal and ethical basis for medical treatment of a patient in extremis with no available surrogate decision-maker.
Implied/emergency consent
(delay would pose risk of serious, imminent harm)
500
In auto-PEEP or breath stacking with hemodynamic instability, this maneuver should take first priority.
Disconnect the ventilator circuit and manually push the air out of the chest
500
A complication that develops when plateau pressures of 40 cmH₂O and PEEP of 35 are sustained for 72+ hours in a patient with ARDS.
Pulmonary fibrosis
500
Pulmonary edema developing after multiple blood transfusions--that does not respond to diuresis--is most consistent with this diagnosis.
TRALI (transfusion-related acute lung injury)
500
Blood cultures may not be needed for patients presenting with this type of pneumonia.
Non-severe community acquired pneumonia
500
Hospital-acquired and ventilator-acquired pneumonias have a stricter definition than community-acquired pneumonia. All four of these elements are required for diagnosis.
- New infiltrate on chest imaging
- Respiratory decline
- Fever
- Productive cough
500
This calculation can help predict the success of extubation.
Rapid shallow breathing index
(resp rate/tidal volume ≤ 105)
500
The thick walled lucency in the left apex is concerning for this infection, among others.
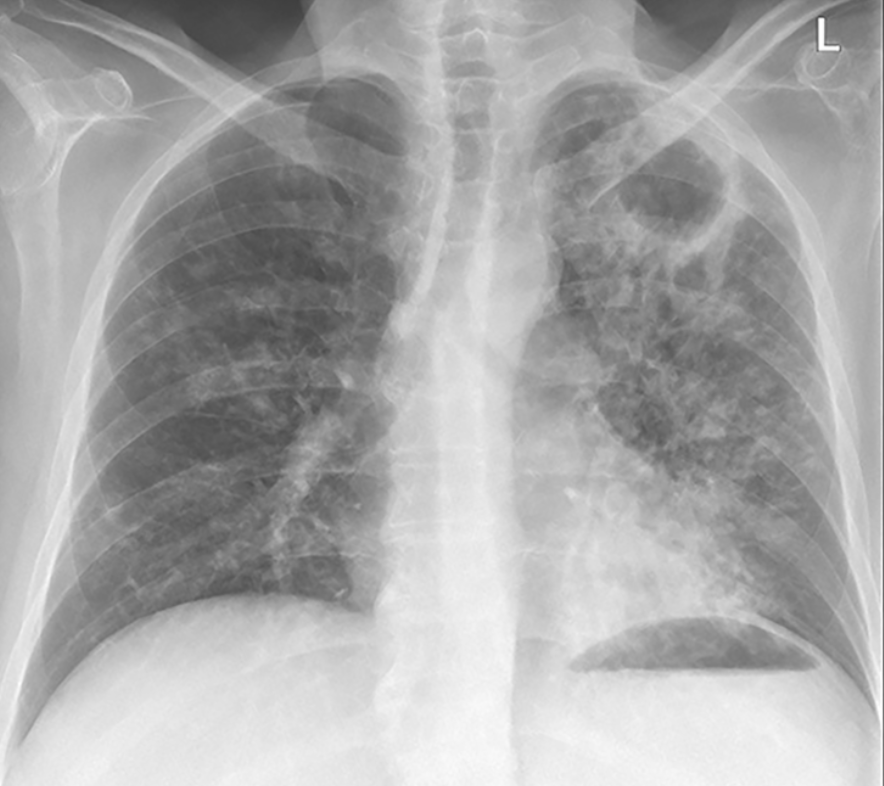
Pulmonary M tuberculosis infection