Name That Biologic
Imaging Clues
Arthritis/Myopathies
Autoimmune/Connective Tissue Diseases & Vasculitis
100
A 37-year-old woman comes to the physician with pain in her hand joints lasting several months. She feels she is clumsy in the morning because her hands are stiff and tender. Four weeks ago the patient was treated for knee pain and swelling with naproxen. Her past medical history is otherwise unremarkable.
Joint examination shows warmth, swelling, and tenderness in the proximal interphalangeal and metacarpophalangeal joints and both wrists. X-rays show periarticular osteopenia and erosions of the proximal interphalangeal and metacarpophalangeal joints.
Laboratory results are as follows:
Hemoglobin11.4 g/dLMean corpuscular volume86 fLLeukocytes4,100/µLCreatinine0.8 mg/dLC-reactive protein27 mg/LRheumatoid factor90 U/mLAnti-nuclear antibodyNegative
The patient is treated with nonsteroidal anti-inflammatory therapy with significant symptomatic relief.
Which of the following is the most appropriate next step in management of this patient?
A. Etanercept
B. Low-dose maintenance prednisone
C. Methotrexate
D. Rituximab
E. Sulfasalazine
C. Methotrexate
100
A 65-year-old man comes to the physician due to attacks of joint pain and swelling that affect primarily his hands but sometimes his knees or elbows. He currently has no pain, but the episodes occur once or twice a month.


Which of the following agents is most likely to provide long-term relief for this patient's symptoms?
A. Allopurinol
B. Etanercept
C. Methotrexate
D. Prednisone
E. Sulfasalazine
A. Allopurinol
100
A 32-year-old man is evaluated for a 4-month history of progressive polyarticular joint pain. He experiences morning stiffness lasting 45 minutes. His only medication is ibuprofen, which he has been taking three times daily for the past month.
On physical examination, vital signs are normal. Swelling and tenderness of the second and fourth metacarpophalangeal joints, wrists, knees, and ankles are present bilaterally. Tenderness on compression of the metatarsophalangeal joints in both feet is noted. No rashes or skin changes are observed.
Which of the following will most likely confirm the diagnosis?
A. Antinuclear antibodies
B. C-reactive protein and erythrocyte sedimentation rate
C. HLA-B27 antigen
D. Rheumatoid factor and anti–cyclic citrullinated peptide antibodies
D. Rheumatoid factor and anti–cyclic citrullinated peptide antibodies
100
A 30-year-old woman comes to the physician with the complaint of cold hands. Symptoms occur during winter months or when she reaches into the freezer at home. The coldness is often associated with intense pallor and a bluish color. On recovery, the hands feel warm and appear red and flushed. With severe attacks, the patient has numbness and tingling in the hands. On rare occasions, she can also feel the sensation in her toes. She denies skin rashes, joint pain, acid reflux, dyspnea, or chest pain.
She has no other medical problems and takes no medication. Family history is unremarkable. She does not use tobacco, alcohol, or illicit drugs.
Her blood pressure is 122/70 mm Hg and pulse is 78/min. Lungs are clear on auscultation. No bruits are heard in the periumbilical area. Peripheral pulses are symmetric and full. Skin examination is normal.
Which of the following is the best next step in this patient’s evaluation?
A. Ankle brachial index
B. Carotid duplex ultrasound
C. Dilated fundus examination
D. Monofilament testing
E. Nail bed capillaroscopy
E. Nail bed capillaroscopy
200
A 36-year-old man with known ankylosing spondylitis for the last 7 years comes to the physician complaining of persistent back pain. He describes aching pain at night and in the morning that slowly goes away during the day. In the evening, he feels fine and prefers to do most of his activities then. He takes high-dose naproxen, which previously relieved his pain but recently has had only moderate effect. He was evaluated for right hip pain 6 months ago, but no joint involvement was diagnosed.
His vital signs are within normal limits. Examination shows limited spinal mobility and sacroiliac joint tenderness.
Laboratory results are as follows:
Hemoglobin 10.5 g/dL
Platelets 350,000/µL
Creatinine 0.8 mg/dL
C-reactive protein11 mg/dL (N: < 0.3 mg/dL)
Which of the following is the best next step in managing this patient?
A) Adalilumab
B) Methotrexate
C) Prednisone
D) Sulfasalazine
A) Adalilumab
200
A 65-year-old woman comes to the physician with a rash on her hands for the past 2 weeks. Two months ago she developed a rash on her face and forearms while vacationing at a beach resort. Her review of systems is positive for recent onset weakness of the shoulders and hips. Upper and lower limb deep-tendon reflexes are 2+. She has difficulty rising from a chair. Muscle strength is 4/5 in both upper and lower extremities.
Laboratory results are as follows:
Serum creatine kinase1040 U/L
Anti-nuclear antibody (ANA)1:160,
Erythrocyte sedimentation rate 68 mm/h

This patient would require which of the following?
A) Anti dsDNA antibody screening
B) Low Dose Prednisone
C) Cancer screening
D) Liver Biopsy
C) Cancer screening
200
A 52-year-old man comes to the physician for intermittent sore throat, nocturnal high fevers, cold sweats, fatigue, anorexia, and weight loss over the last 4 weeks. He also complains of pain and swelling of his hands and wrists and brief episodes of a rash. He does not recall any tick bites and has no travel history or ill contacts. His temperature is 39 C (102.2 F), blood pressure is 100/70 mm Hg, and pulse is 92/min. Oropharyngeal mucosa is dry without exudates. There are several enlarged cervical lymph nodes. A scarce macular, nontender, purple rash is noted on both arms. There are no heart murmurs. Splenomegaly is noted. Synovitis is present in several joints including both hands, wrists, and elbows. A moderate effusion is present in the left knee joint. Laboratory results are as follows:
Hemoglobin 9.5 g/dL
Platelets 620,000/µL
Leukocytes 18,500/µL
Creatinine 0.8 mg/dL
C-reactive protein 12 mg/L
Erythrocyte sedimentation rate 112 mm/h
Rheumatoid factor 15 U/mL
Cyclic citrullinated peptide antibodies Negative
Serum ferritin 8430 ng/mL
Which of the following is the most likely diagnosis?
A) Adult-Onset Still's Disease
B) Felty Syndrome
C) Sweet Syndrome
D) Post-Streptococcal reactive arthritis
A) Adult-Onset Still's Disease
200
A 72-year-old man comes to the physician because of shoulder pain, which has been present for 3 weeks and began after a mild fall that was braced by his outstretched arm. The pain is felt over his lateral shoulder and often keeps him awake at night. It also makes it difficult for him to lift anything overhead.
Passive range of motion is normal; however, range of motion with any resistance is limited and the patient is unable to maintain 90 degrees of abduction. There is weakness with abduction and external rotation.
Which of the following is the most likely diagnosis?
A. Cervical nerve root impingement (1%)
B. Frozen shoulder
C. Osteoarthritis
D. Rotator cuff impingement
E. Rotator cuff tear
E. Rotator cuff tear
300
A 25-year-old woman is seen in the office for ongoing management of rheumatoid arthritis, which was diagnosed 1 year ago. Oral methotrexate was initiated after diagnosis; the dose was subsequently increased to the current dose of 25 mg orally weekly and switched to subcutaneous administration. She experiences approximately 24 hours of pronounced fatigue and decreased appetite following each dose of methotrexate but has no other adverse effects. Her other medication is folic acid, 1 mg/d. Contraception consists of a copper intrauterine device.
On physical examination, vital signs are normal. No active joint swelling or tenderness is observed.
Laboratory studies show normal complete blood count, serum electrolyte levels, serum creatinine level, and liver chemistry panel.
Which of the following is the most appropriate treatment?
A. Add adalimumab
B. Add vitamin D
C. Change methotrexate dosing from weekly to daily
D. Discontinue methotrexate
E. Increase folic acid
E. Increase folic acid
300
A 35-year-old woman comes to the physician for a follow-up visit. She was recently diagnosed with systemic lupus erythematosus after a 2-month history of fatigue and a skin rash. She was advised to use over-the-counter hydrocortisone cream for the facial rash but it did not help. Her previous medical history is insignificant. The patient has never been pregnant. She does not use tobacco and drinks only 1 or 2 alcoholic beverages a week. She currently takes no prescription medications.
Her vital signs are normal. Skin findings are shown in the image below.

Which of the following is the best therapy for this patient's rash?
A. Dapsone
B. Hydroxychloroquine
C. Isotretinoin
D. Lenalidomide
E. Methotrexate
B. Hydroxychloroquine
300
Name five bacterial pathogens that commonly precede reactive arthritis
Chlamydia trachomatis, Salmonella, Shigella, Campylobacter jejuni, and Yersinia enterocolitica.
300
Malignancies associated with dermatomyositis
- Adenocarcinoma (eg, lung, breast, ovarian)
- Lymphoma
400
A patient with an acute osteoporotic vertebral compression fracture has persistent pain despite NSAIDs and acetaminophen. Which medication is associated with the improvement of acute fracture-related pain when given shortly after fracture?
Nasal calcitonin
400
A 52-year-old man comes to the physician with a week of pain and discoloration of his fingers. He has had profound fatigue and diffuse arthralgias for the past 6 months. He has not had any weight loss, fever, chills, hematuria, cough, hemoptysis, or shortness of breath. He has a history of asthma, intravenous drug use, depression, and peptic ulcer disease. He smoked 2 packs per day for 20 years but quit 10 years ago. He drinks occasionally but has not used intravenous recreational drugs for more than 10 years. He works as an auto mechanic.
On examination, the right hand appears as shown below. The remainder of the physical examination is unremarkable.

Complete blood count:
Hemoglobin 13.5 g/dL
Platelets 340,000/mm3
Leukocytes 9,100/mm3
Serum creatinine 1.0 mg/dL
Urine protein trace
Immunologic and rheumatologic studies:
Anti-nuclear antibody1:160
Complement C356 mg/dL (normal: 83-177) C45 mg/dL (normal: 16-47)
Rheumatoid factor 560 U/mL (normal: <15 U/mL)
Which of the following is the most likely diagnosis?
A. Buerger disease
B. Cholesterol emboli syndrome
C. Churg-Strauss syndrome
D. Hepatitis C infection
E. Primary Raynaud phenomenon
D. Hepatitis C infection
400
A 52-year-old man with a history of rheumatoid arthritis comes to the clinic due to increasing pain and swelling involving several joints over the past 6 weeks. The patient also has fatigue and morning stiffness that can last for hours. He was diagnosed with rheumatoid arthritis 2 years ago after he presented with symmetrical polyarthritis, a high-titer rheumatoid factor, and positive cyclic citrullinated peptide antibodies. Treatment with methotrexate and nonsteroidal anti-inflammatory agents resulted in reduction of joint pain and swelling. At his last visit 3 months ago, the patient had only mild joint pains without any morning stiffness. His other medical problems include hypertension, diverticulosis, and hyperlipidemia.
His temperature is 37.4 C (99.4 F), blood pressure is 135/82 mm Hg, and pulse is 77/min. Gentle squeezing of his hands and feet evokes pain. Several small joints of the fingers and toes are swollen and tender. There is mild boggy swelling of the left knee. Subcutaneous nodules are seen over the elbows. The remainder of the physical examination is unremarkable.
Laboratory results are as follows:
Hemoglobin 10.4 g/dL
Platelets 450,000/mm3
Leukocytes 9,200/mm3
Creatinine, serum 0.9 mg/dL
Erythrocyte sedimentation rate 67 mm/h
Which of the following is the best next step in management of this patient?
A. Arrange for skin tuberculin testing
B. Check antineutrophil cytoplasmic antibody levels
C. Check Lyme disease titers
D. Stop methotrexate and observe
E. Stop methotrexate and start sulfasalazine
A. Arrange for skin tuberculin testing
400
Five criteria effective for distinguishing giant cell arteritis from other vasculitides

500
A 42-year-old woman is evaluated for dyspnea on exertion. She has a 2-year history of anti–Scl-70–positive diffuse cutaneous systemic sclerosis. Previously, she could walk 1 mile without stopping, but she now requires a 10-minute rest halfway through. Medications are nifedipine and pantoprazole.
On physical examination, respiration rate is 16/min and oxygen saturation is 95% with the patient breathing ambient air. Other vital signs are normal. Lung examination demonstrates bibasilar crackles. Cardiac examination is normal. Skin tightening is observed on the hands, forearms, chest, and forehead.
High-resolution CT scan demonstrates basilar predominant reticulation and scattered ground-glass opacities. Pulmonary function studies showed 10% decline in FVC or 15% decline in Dlco within 12 months
Which of the following is the most appropriate treatment?
A. Cyclosporine
B. Methotrexate
C. Mycophenolate mofetil
D. Prednisone
C. Mycophenolate mofetil
500
A 72-year-old woman is evaluated for chronic right shoulder pain associated with a large effusion.
A radiograph of the right shoulder is shown.
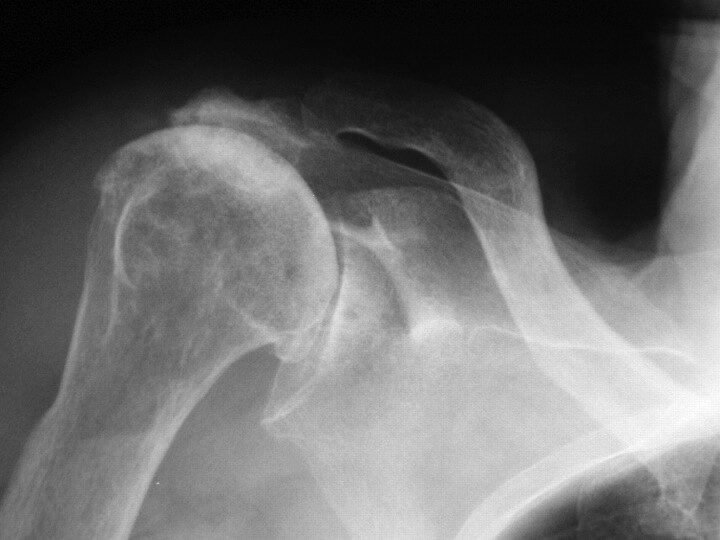
A. Basic calcium phosphate deposition
B. Calcium pyrophosphate deposition
C. Osteoarthritis
D. Rheumatoid arthritis
A. Basic calcium phosphate deposition disease (Milwaukee shoulder)
500
A 70-year-old man comes to the physician with muscle pains and weakness over the last several weeks. He now has difficulty getting up from a chair and climbing stairs. He has no fever, weight loss, vision changes, or shortness of breath.
The patient’s other medical problems include hyperlipidemia, gout, hypertension, chronic kidney disease, and degenerative joint disease of the hips and knees. His medications include lisinopril, allopurinol, colchicine, atorvastatin, and acetaminophen.
Vital signs are within normal limits. Examination shows some tenderness to palpation of his thighs and weakness of both thighs to extension and flexion. Deep-tendon reflexes are symmetrically diminished at the patellar tendons and absent at the Achilles tendons. Peripheral pulses are normal.
Laboratory results are as follows:
Creatine kinase 1200 U/L
Anti-nuclear antibody Negative
C-reactive protein 8 mg/L
Erythrocyte sedimentation rate 17 mm/h
Electromyogram shows slowed sensory and motor nerve conduction velocities and small-amplitude, short-duration polyphasic waves.
A quadriceps muscle biopsy demonstrates widespread cytoplasmic vacuolization but no inflammation.
What is the most likely explanation for this patient’s symptoms?
A. Atorvastatin
B. Colchicine
C. Diabetic amyotrophy
D. Hypothyroidism
E. Polymyositis
B. Colchicine (Colchicine neuromyopathy)
500
Name antibodies for the following autoimmune diseases:
Systemic sclerosis
Mixed connective tissue disease
Limited Scleroderma
Polymyositis / dermatomyositis
Systemic sclerosis
- RNA polymerase II & III
- Scl-70/anti–topoisomerase type I
Mixed connective tissue disease
- Ribonucleoprotein (RNP) (100%)
Limited scleroderma
- Centromere
Polymyositis, dermatomyositis
- Aminoacyl-transfer RNA synthetases (eg, Jo-1)