Pressure Injury
Skin Care
Product Selection
Documentation
Prevention
100
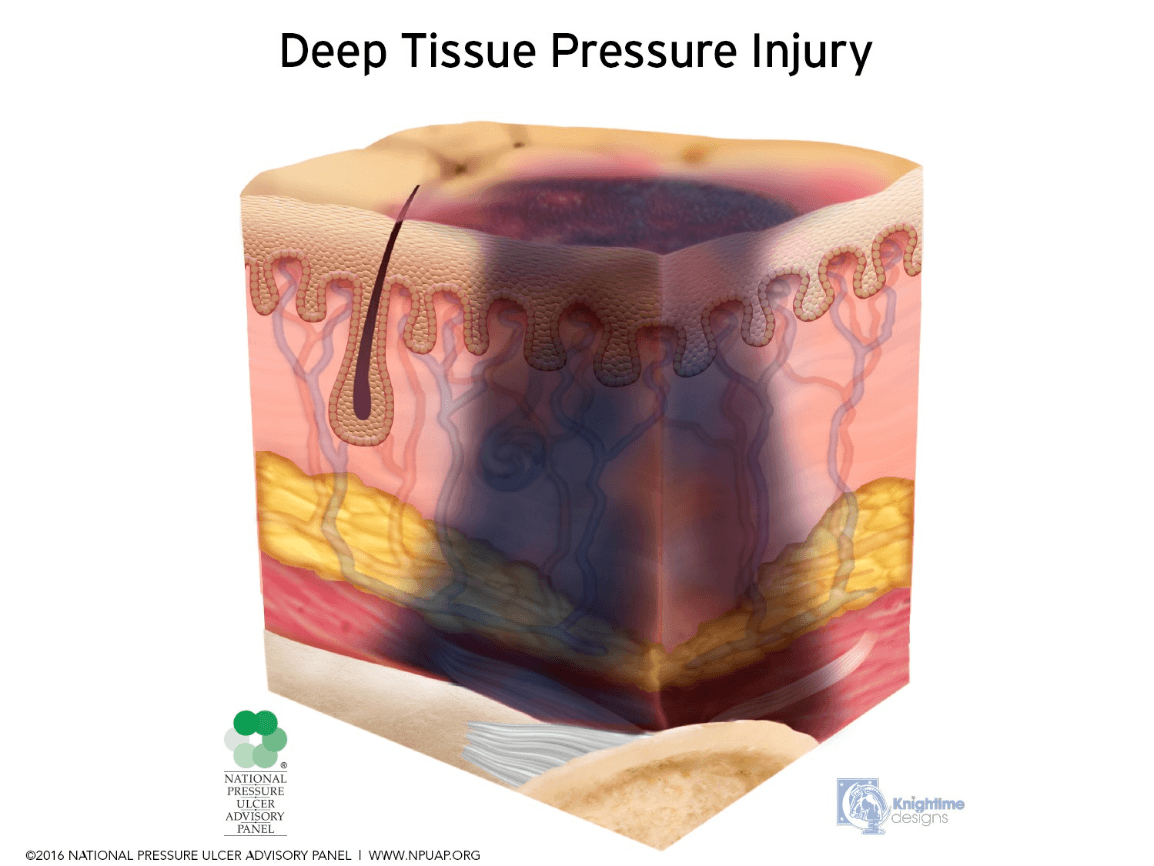
The skin may be purple or maroon localized area of discolored intact skin or a blood filled blister.
What is a Deep Tissue Injury?
100
Must be conducted by the RN at least every 24 hours
What is a Skin Assessment?
100
Is used during the first step in wound treatments.
What is a wound cleanser?

100
linear scratches found on the skin
What is excoriation?


100
To inspect, protect and secure the skin.
What is Skin Injury Prevention?
200
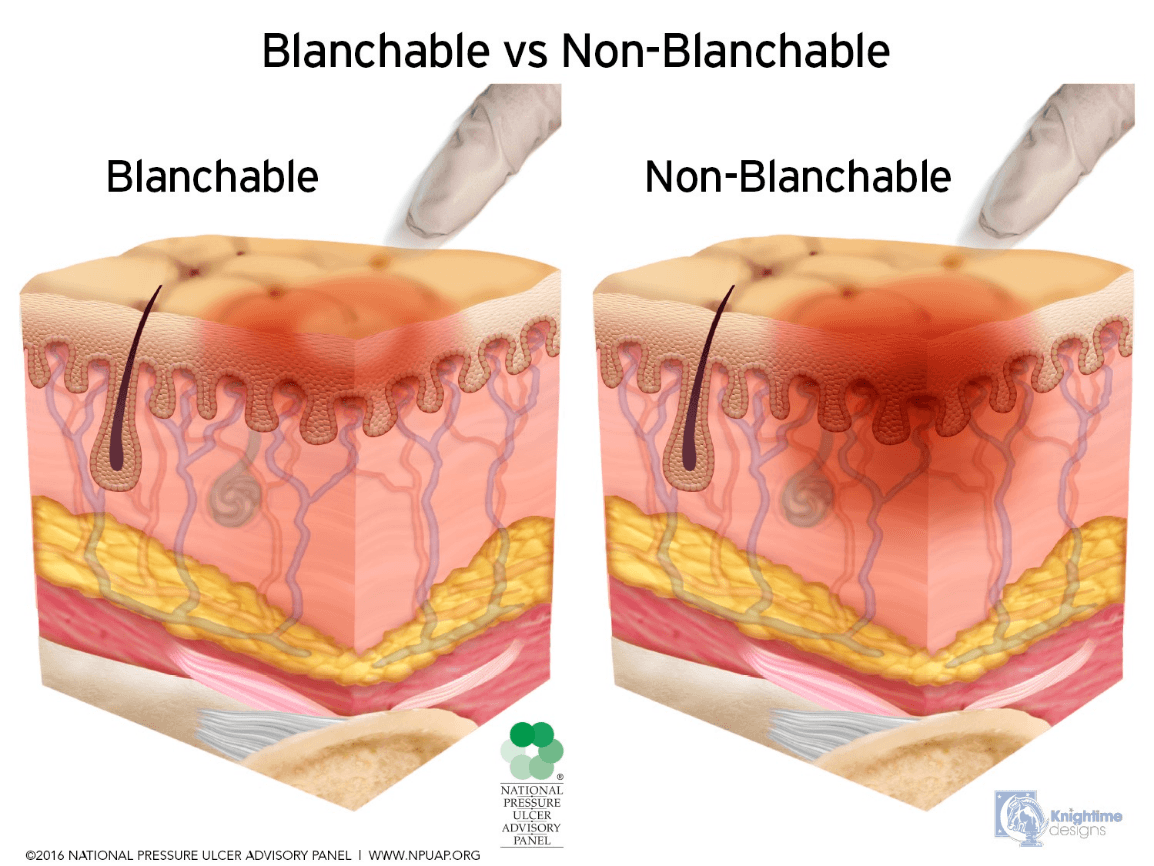
The skin is intact and has blanchable redness.
What is not a pressure injury?
200
A nurse performs this task when a patient is diapered.
What is application of a moisture barrier?
200
The product that is placed directly on a wound.
What is a primary dressing?
200
Measurement used to describe the size of the wound.
What is Length x Width x Depth? (in centimeters)

200
Used mainly in the NICU and PICU for babies that cannot reposition.
What are gel rolls or gel pads?

300
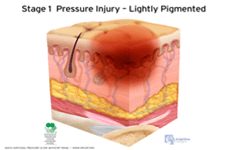
Skin is intact with non-blanchable redness of a localized area. Usually over a bony prominence.
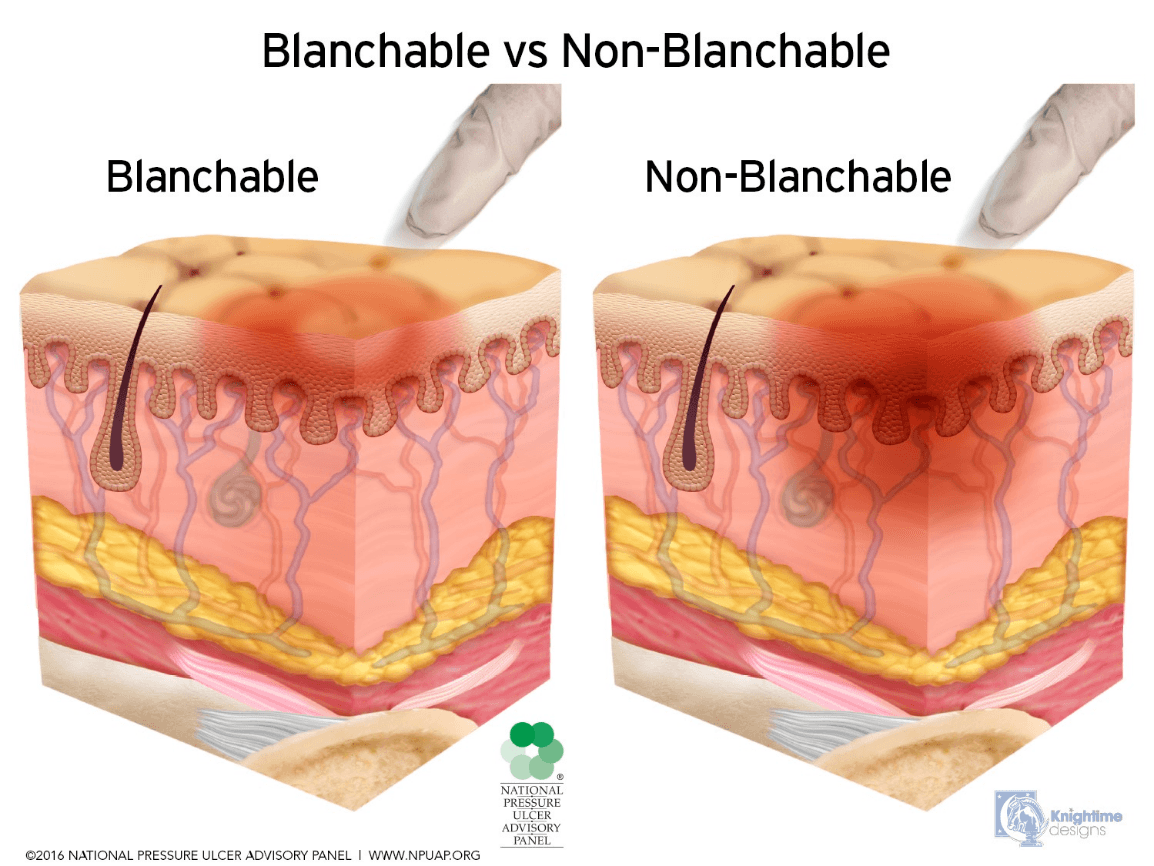
What is a Stage 1 pressure injury?
300
Is used when a patient has reddened, open or denuded skin.
What is Z-Guard?

300
Is used to help control drainage, stimulates tissue growth and over surgical incisions?
What is Negative Pressure Wound Therapy?
300
The excess of new connective tissue with tiny blood vessels presents by secondary intention in wound healing
What is hypergranulation tissue or proud flesh?
300
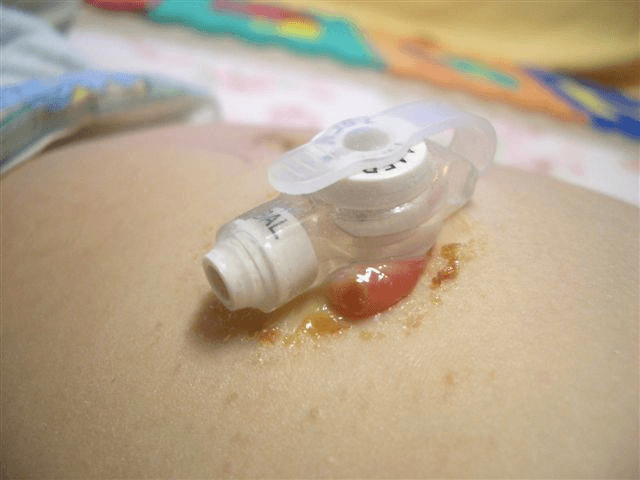
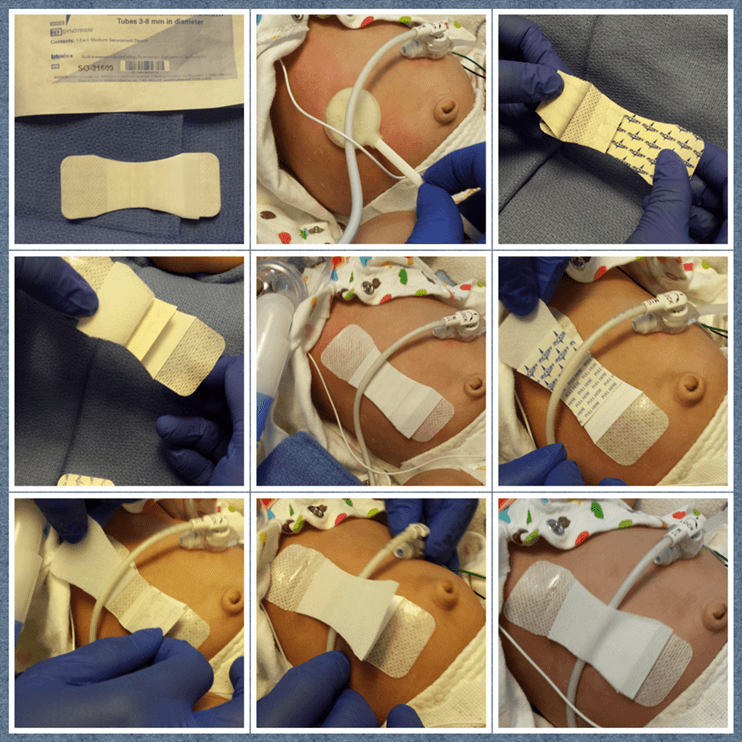
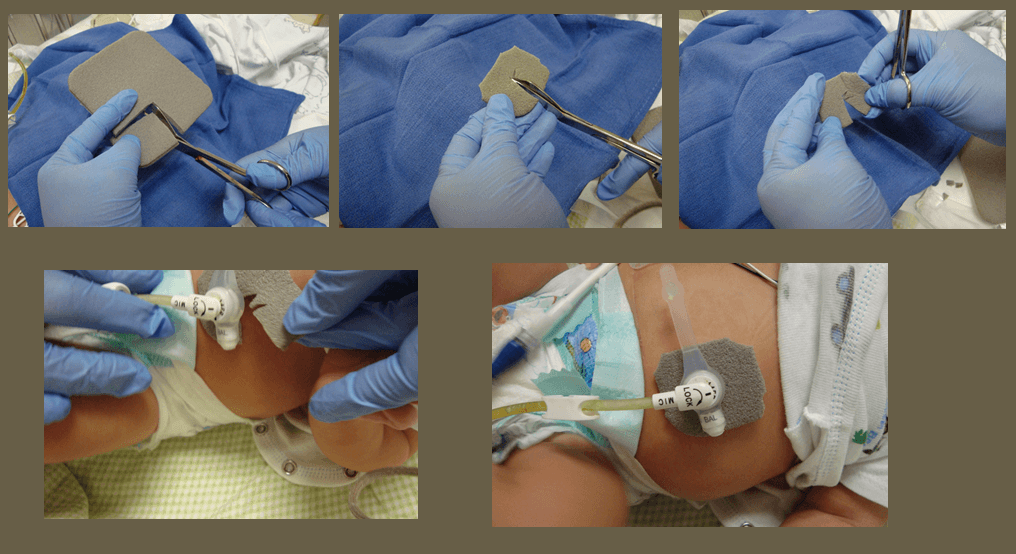
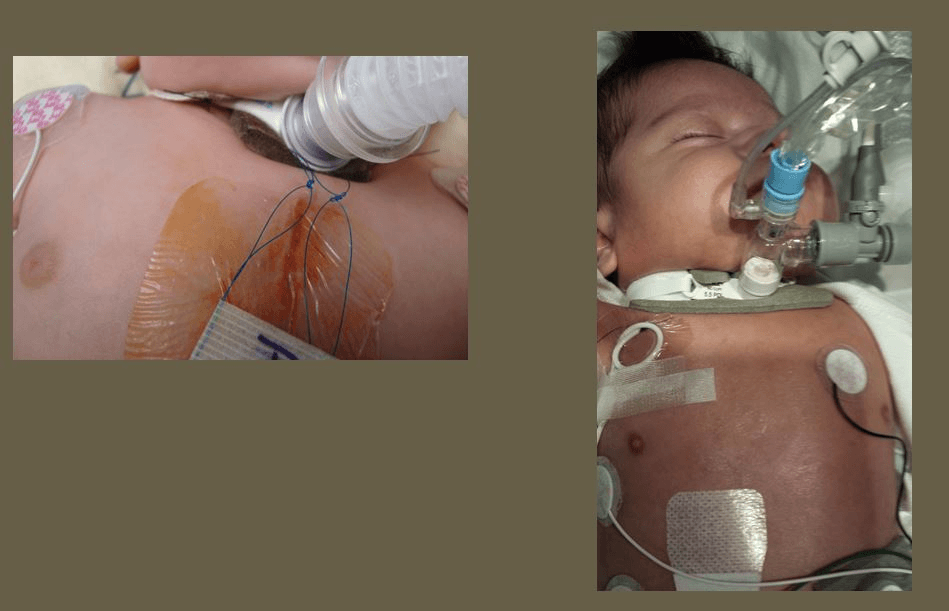
Is used to stabilize tubing from pulling or tugging and creating damage to skin.
What is a securement device?
400
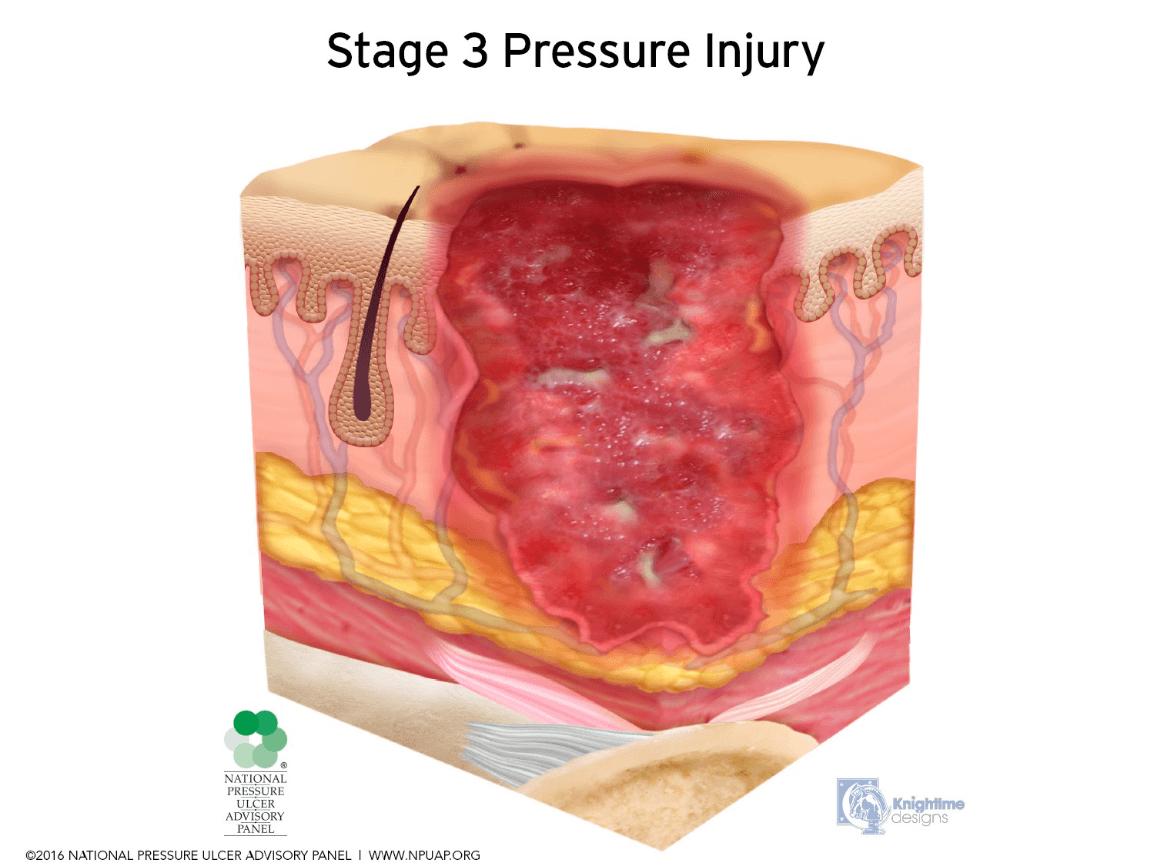
Full thickness tissue loss where bone, tendon or muscle are NOT exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling.
What is a Stage 3 pressure injury?
400
Are used as a tool to assess the risk of skin breakdown.
What are the Braden, Braden Q and NSCS?
400
Has antimicrobial property, wear time is up to 7 days and can be used on G-tube sites, trach sites and burns?
What is Mepilex Ag foam?

400
Is written by the Wound Care Nurse Practitioner to communicate wound care management.
What is an order or nursing communication?
400
Is found under newly placed trachs and gtubes.
What is Mepilex Ag foam?
500
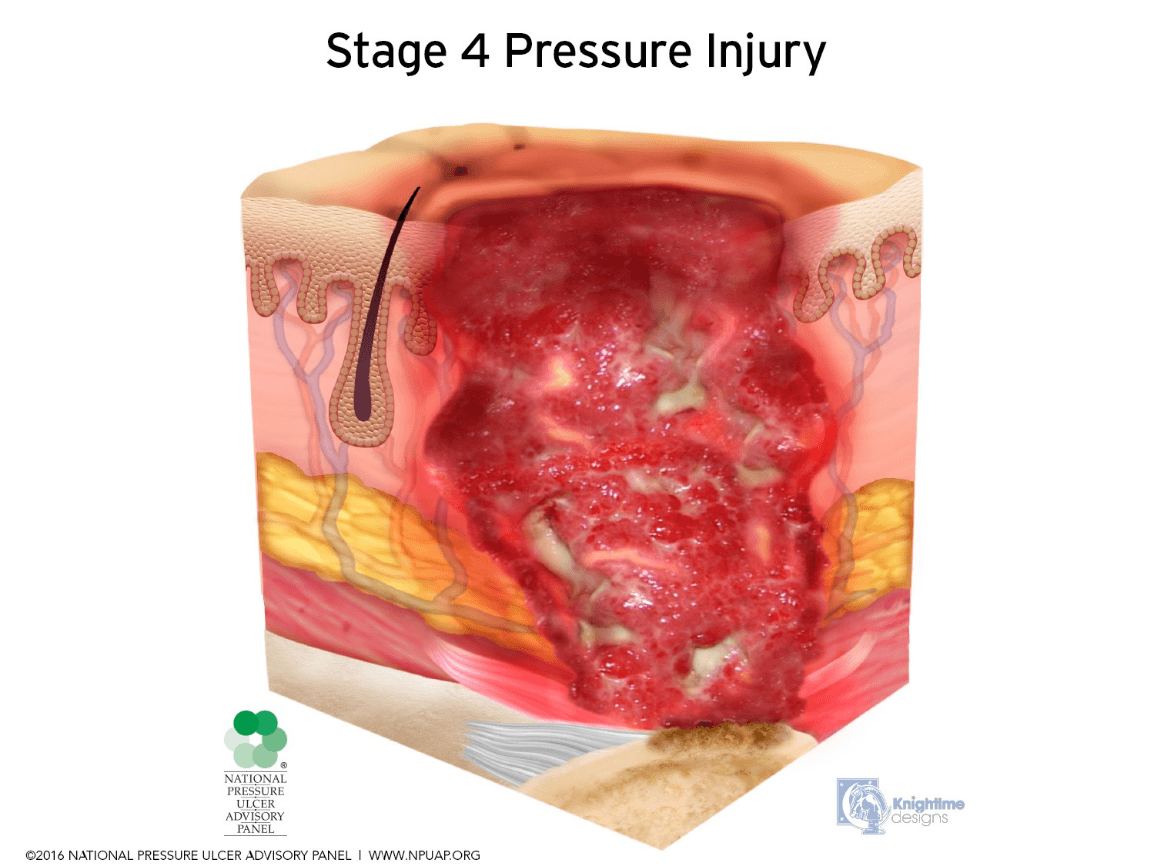
Full tissue loss with exposed bone, tendon or muscle. Often will include undermining and tunneling.
What is a Stage 4 pressure injury?
500
Upon admission and the skin assessment, the nurse identifies a pressure injury.
What is present on admission POA?
500
The product that is placed on a wound to secure or cover the primary dressing.
What is a secondary dressing?

500
Are used to communicate Wound Assessment and Recommendations/Plan by the Wound Care NP.
What is a Wound Care Consult Note and Wound Care Progress Note ?

500
A bed surface used to help with Stage 3 and Stage 4 pressure injury.
 What is a pressure redistribution mattress?
What is a pressure redistribution mattress?
600
Wound Care NP will stage pressure injuries.
Nurses should document according to color and tissue type. Blanchable or Non-blanchable redness. Use red, green yellow, black, brown tissue.
Residents and physicians place a wound care consult.
 Who stages pressure injuries?
Who stages pressure injuries?
600
The optimal pH of human skin.
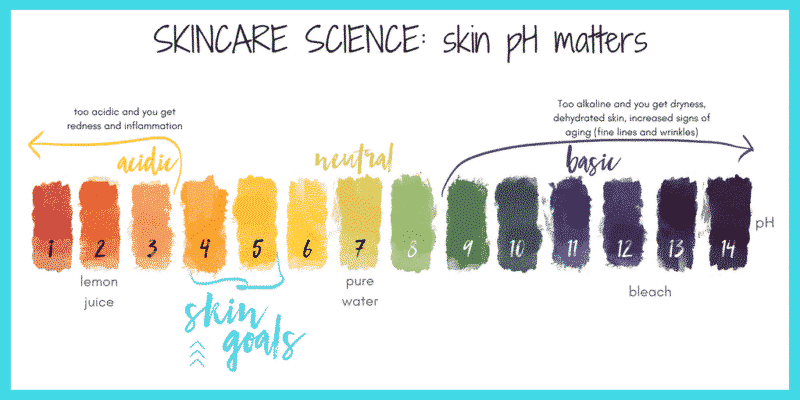 What is 5.5 ?
What is 5.5 ?
600
A wound dressing NOT used when too much drainage is requiring frequent changes.
What is a 7 day dressing?

600
Nursing Documentation initiated to document a wound.
What is an LDA?
600
The Skin Team Motto.
What is Prevention is Critical?
