One Stop Shock
Razzle-dazzle Heart Rhythm
Heart Smarts
Cataclysm Cardiac
Lub-Dub Club
100
What are major signs of Hypovolemic shock?
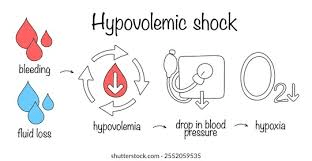
Radical depletion of electrolytes Na, K
Low HGB
Low B/P, High HR
Hypoxia
100
Identify ME
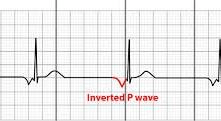

Junctional Rhythm
100
Tell me with TRIK represents in PCI failure?
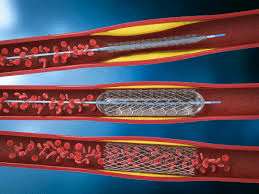
T= Thrombosis
R= Restenosis
I= Infection
K= Kidney damage
100
Explain little CATI in watching your CVP line?
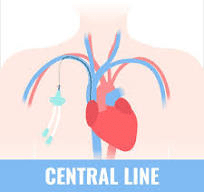

C= Clotting
A= Air embolism
T= Thrombosis
I- Infection
100
Explain disseminated intravascular coagulation (DIC).
What is one thing that causes DIC?
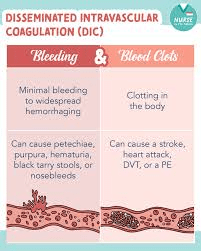
It is like a clotting hurricane that uses up all of the resources. Blood clotting goes into overdrive.
Then you end up clotting and bleeding all at the same time gone Wild.
Sepsis is a major cause for DIC
200
Why do we use CVP monitors?
What type of shock would they work well with?
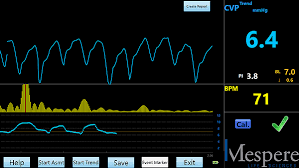
Normal ranges 2-6
ITS ALL ABOUT FLUID MONITORING
Hypovolemic Shock
200
1.
2. 
3.
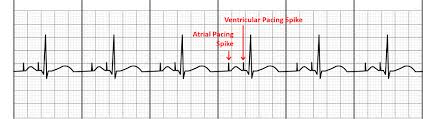
1. A paced
2. AV paced
3. V paced
200
You receive a STAT lab result of a Potassium of an 8. What are the first things you would do?
Assess client
STAT EKG
200
How do you administer amiodarone by IV drip?
What must you know about this med for safety?

We never shake it up
We always have a filter
It is always just titrated one time.
200
Explain to me the nursing care if you are maintaining a cardiac drip? THE RULE OF 2!!!!!
You Titrate slow, never stop it abruptly!
Vitals every 15 minutes.
300
I get a rattle in my spine.
The sympathetic nervous system shows decline
My vitals all start to go hypo
Who am I BRO?

Neurogenic Shock
Low Temp, Low B/P and bradycardia with the HR.
- Massive Vasodilation: Without the SNS telling them to stay constricted, your blood vessels suddenly relax and widen (vasodilation).
- Blood Pooling: Because the vessels are so wide, blood "pools" in your extremities (arms and legs) instead of flowing back to the heart.
- Result: This creates a massive drop in pressure because there isn't enough "squeeze" in the system to move blood effectively to your brain and organs
300
My PR interval gets longer each time
Until my QRS falls off the line
Wenckebach
Second Degree Type Mobitz 1
300
Identify me and what do you feed me?
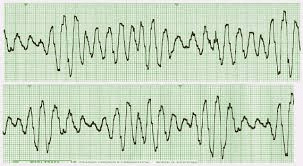
Torsade's De Pointes
Magnesium Sulfate
300
I have a fever night sweats and fatigue
My valves are infected oh poor me
My heart is going weaker from firmer
I also have a new heart murmur.
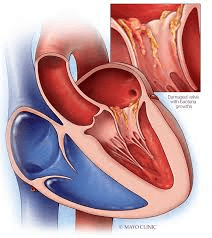
Endocarditis
So, with the fever and proof of infection this is probably infective endocarditis.
300
A nurse receives a new client in ER at shift change with abnormal skin spots and bleeding. The doc that is leaving gave dx of immune thrombocytopenic purpura (ITP) with orders. Which orders do you question?
1. IM morphine
2. Start 2 large IV bores
3. Tylenol
4. IV Toradol

No NSAIDS
NO sticks or anything that causes bleeding.
400
What causes the heart to develop cardiogenic shock?
MUSCLE DAMAGE!
Then the heart loses contractility and the ability to contract Jack!
400
Identify this Strip and tell me what we avoid with this type of Rhythm?
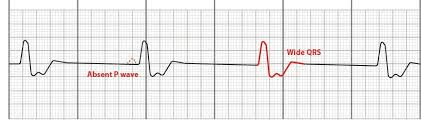
Idioventricular
We avoid negative inotropes!!!
What are they?
400
Identify me

My PR does not change
But my R to R is really deranged
and I can't keep track of the QRS falling back
Second Degree Type 2
400
Client troponin is a 4 and the nurse sees this on the monitor and client complains of 9/10 heart ache.
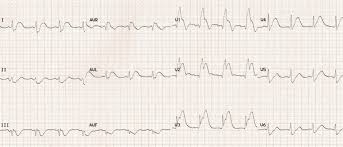
STEMI
400
What do we avoid in HIT (Heparin induced Thrombocytopenia)?
ALL heparin products!!!!
Warfarin in the acute phase because it rapidly depletes Protein C, a natural anticoagulant. In the already hypercoagulable state of HIT, this imbalance can lead to catastrophic microvascular thrombosis, causing skin necrosis or venous limb gangrene.
IM injections
Platelet transfusions generally contraindicated in acute/subacute HIT because they provide more targets for the HIT antibodies, which can worsen thrombosis, unless the patient is experiencing severe, life-threatening bleeding.
500
What shock is heavily related to body temp and can be a high or low. We check to see if the body is going to plan B and check the lactic acid and get ready for fluids on the rapid?
What is the gold standard med we give?
Septic Shock
Levo Norepinephrine
500
Identify me:

My PR interval is strange with a change
But don't be a fool the R to R is the still cool
I look okay but the p's and q's are in a fight
It must be a 3rd degree night!
500
Explain why in Acute decompensated heart failure why we do not administer a beta blocker?
In patients with Heart Failure with Reduced Ejection Fraction (HFrEF), the heart is already struggling to maintain adequate cardiac output. Negative inotropes, such as certain calcium channel blockers (e.g., verapamil, diltiazem) or beta blockers, can further reduce contractility, potentially triggering acute decompensated heart failure or cardiogenic shock!!!
500
Explain to me why in V-Tach we hold calcium channel blockers?
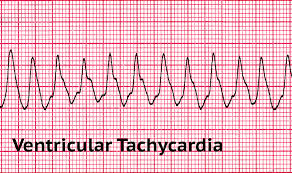
n Ventricular Tachycardia (VT), the heart is already in a state of crisis, beating so fast that it cannot fill with enough blood between beats, leading to low Cardiac Output.
Administering calcium channel blockers (CCBs), such as Verapamil or Diltiazem, during VT triggers "cardiovascular collapse" through three simultaneous physiological hits:
- Profound Negative Inotropy: CCBs block the calcium influx required for the heart muscle to contract. In VT, the heart is already struggling to pump; the CCB further weakens this "squeeze" (contractility), which can lead to immediate Cardiogenic Shock.
500
Tell me the difference in Cardiomyopathy of Hypertrophic and Dilated?
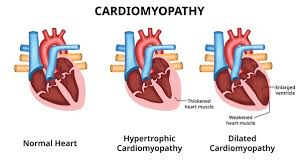
Dilated: ETOH abuse over time heart stretches and becomes harder to pump.
Hypertrophic: Genetic, triggered by exercise new heart murmur and sudden syncope.