You make my heart race <3
Anyone hear about any betting TIPS in the news lately...
No one else was in the rheum where it happened
Board Certified Boards and Beyonder
Please don't make me feel older than I already am
100
What is the difference between a couplet and ventricular bigeminy?
Couplets = 2 consecutive PVCs
Bigeminy = every second beat is a PVC
100
What is definitive treatment for hepatorenal syndrome?
Vasopressor + Albumin
Terlipressin and albumin
Levo and albumin
Midodrine and octreotide and albumin
100
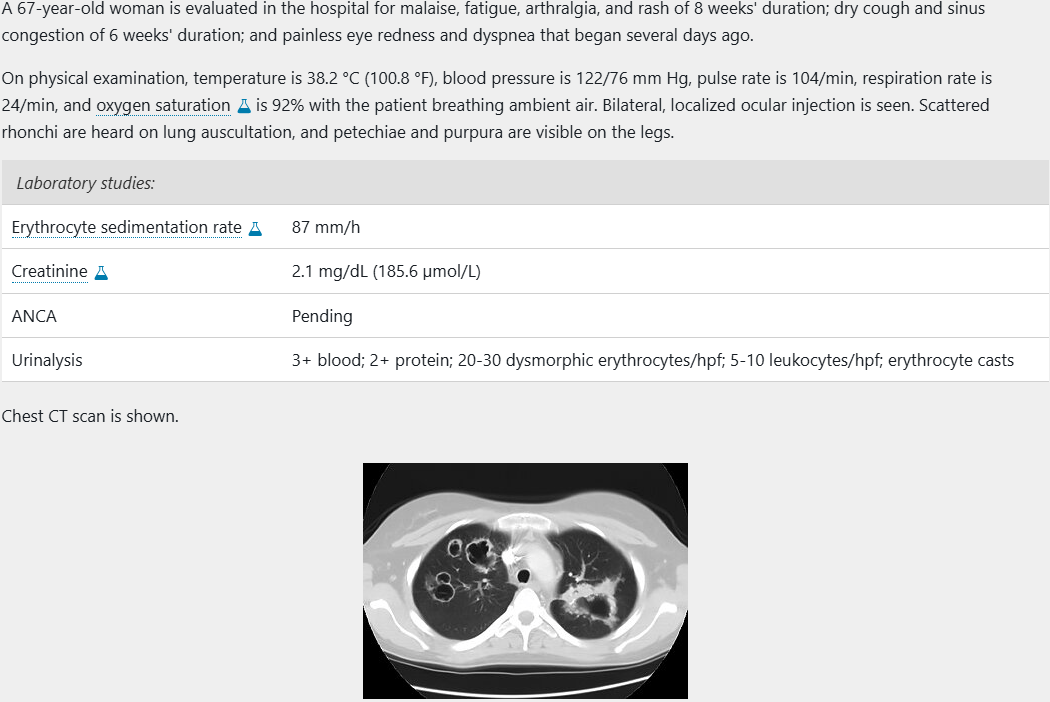 What is the most appropriate diagnostic test to perform?
What is the most appropriate diagnostic test to perform?
Kidney biopsy. Most likely patient has GPA, need a tissue biopsy to confirm prior to starting treatment given the risks of tx (unless dx is clear and there is urgent need for tx). GPA with kidney involvement is expected to have pathognomonic findings
Sinus biopsy is less invasive but poor sensitivity
Skin biopsy would have vasculitic changes but is nonspecific
Lung biopsy might show GPA changes but has a greater morbidity
100
How do you diagnose OHS?
Day time ABG showing hypercapnia and hypoxemia
100

Is mayonaise an instrument?
200
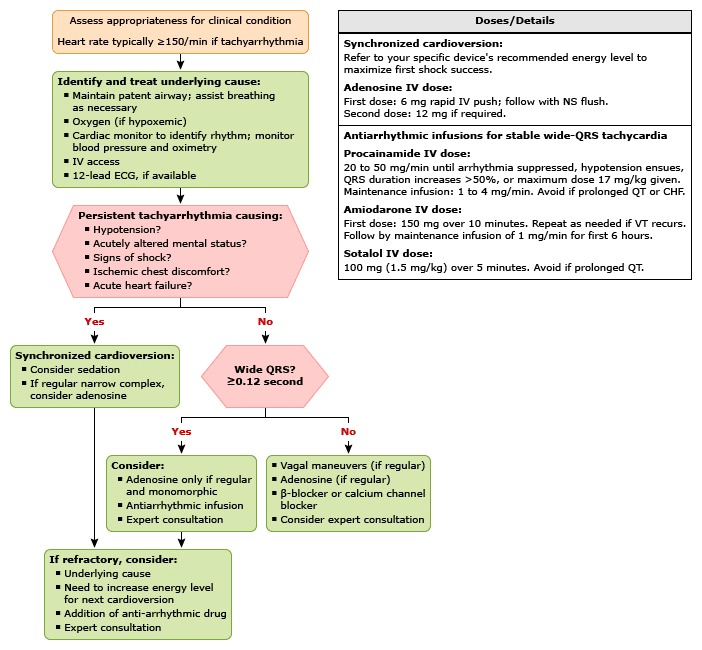
You get called for an RRT for tachycardia! You go through your ACLS algorithm starting with your ABCs, getting EKG, etc. What is the NEXT most important step in the algorithm?
STABLE vs UNSTABLE!
200
Name a cause of pre, intra, and post hepatic portal hypertension
Pre: PVT, splenic vein thrombosis
Intra: Cirrhosis
Post: Budd Chiari, RHF, constrictive pericarditis
200
What drug do you most commonly use in pregnant lupus patients?
Hydroxychloroquine and prednisone
Can technically use azathioprine but avoid unless absolutely necessary
200
You're concerned your patient has a phrenic nerve injury! How do you evaluate for diaphragmatic paralysis?
Sniff test!
Have the patient sniff forcefully under fluoroscopy; a healthy diaphragm moves down while a damaged diaphragm paradoxically moves up
200

"I don't need it, I don't need it.... ______________"
I NEED IT!!!!
300
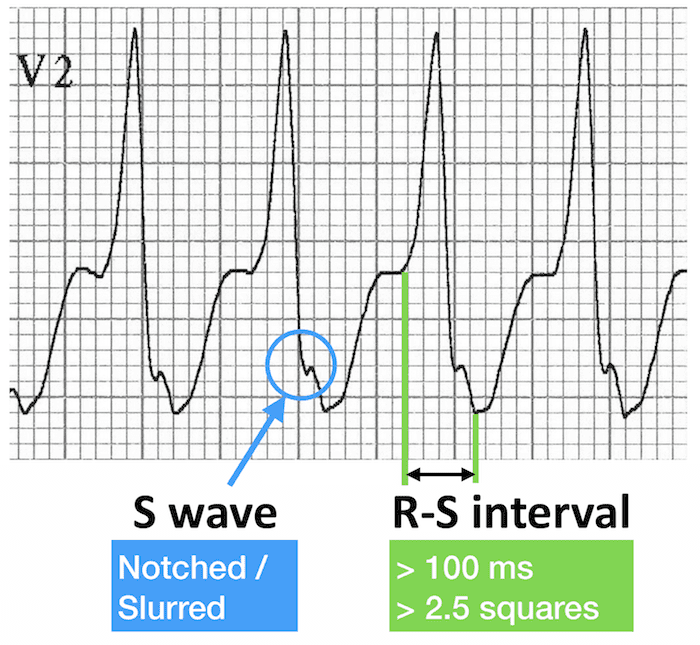
What is the name of this S wave notch and what is its significance?
Josephson Sign, highly specific for VT
300
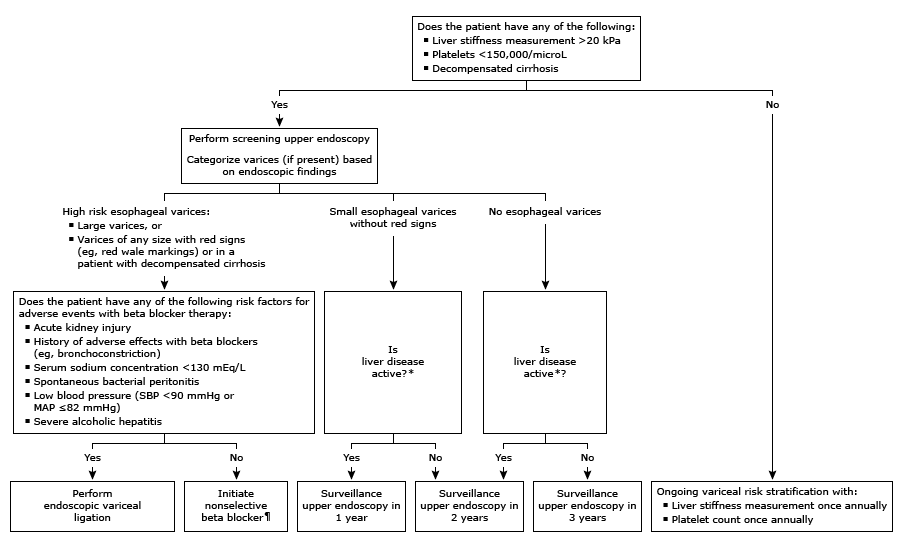
What are your criteria for screening a patient with EGD for EV?
Liver stiffness >20 kPa, Platelets <150k, Decompensated cirrhosis
300
What dose of prednisone and for what length of time should patients have a baseline clinical risk assessment for osteoporosis?
>= 2.5mg/day for >= 3 months
300
Your patient is suffering from depression and recently started an SSRI and is having a good response! However, they are having sexual dysfunction. How do you treat this?
First line is to augment with sildenafil for men with ED or women with anorgasmia. Also can consider bupropion in women
If not responding to SSRI would switch to a second class (bupropion or mirtazapine), SNRIs have similar side effect profile
300

"It's not just a boulder, ______________!"
It's a rock!
400
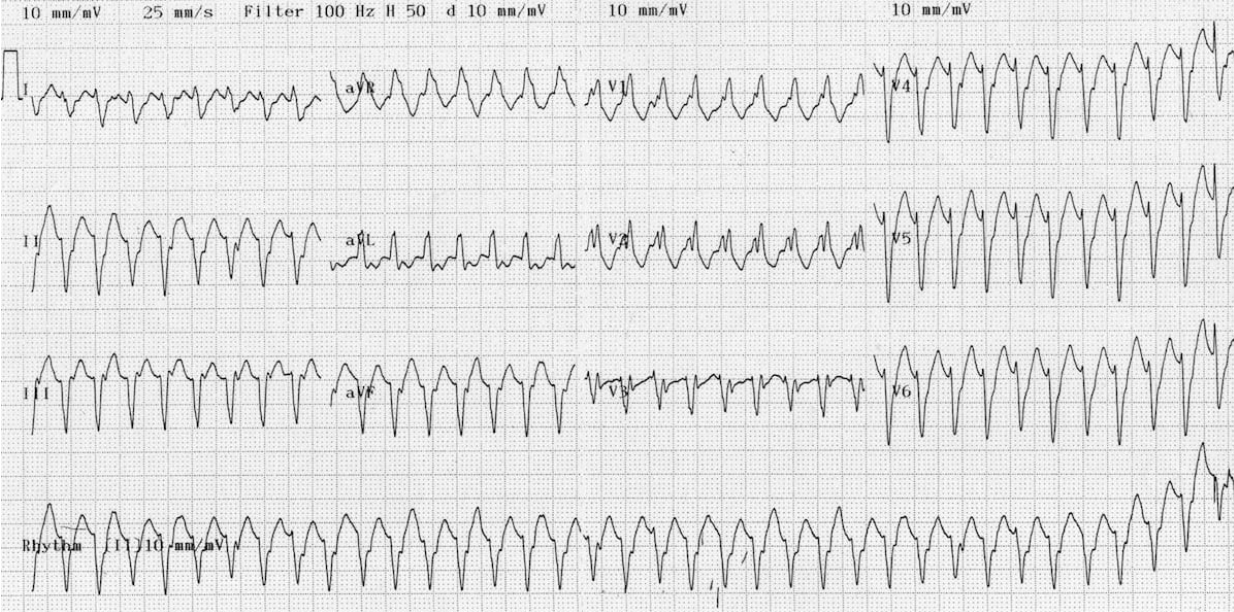
VT!
400
Your patient with cirrhosis weirdly breathes better while lying down and gets hypoxic while sitting up... what is the diagnosis AND how do you diagnose it?
Hepatopulmonary Syndrome
Dx with TTE agitated saline (visualize microbubbles in LA after 3-6 cardiac cycles from RA indicating intrapulmonary shunt)
400
What are 2 criteria for initiating urate-lowering therapy for patients with gout according to ACR?
One or more subcutaneous tophi, evidence of radiographic damage (any modality) attributable to gout, frequent gout flares (two or more annually). CKD3 or more, uric acid level over 9, or urolithiasis are conditional recommendations.
400
You are starting your patient on a statin because their ASCVD meets criteria. What endocrinologic condition should you screen for before initiating and why?
Hypothyroidism as hypothyroid patients have a higher risk of precipitating statin induced myopathy
(impaired metabolism, decreased clearance, impaired muscle regeneration in patients with low thyroid levels)
Tx hypothyroid first, re-evaluate lipids, and then consider starting at a lower dose
400

"Goodbye, everyone, I'll _________"
See you all in therapy!
500
Name the ABCDEs for determining whether a rhythm is VT or SVT with aberrancy
Axis: Extreme Right Axis – 90% specific
Broad Complex: QRS >200ms – 85-90% specific
Concordance: Precordial leads – 97% specific
Dissociation: AV dissociation – Nearly 100% specific
Early part of QRS: RS interval > 100
500
Name 4 contraindications to TIPS
Severe pulmonary HTN, CHF, Severe TR, Active infections, severe coagulopathy, severe hepatic encephalopathy
500
What is the antibody Anti-ribosomal P protein highly specific for?
SLE, particularly in patients with lupus-related psychosis, depression, or renal and liver involvement
500
Your patient presents with an insidious onset of fever, cough, progressive dyspnea, wheezing, weight loss, and night sweats. On lab results, there is peripheral eosinophilia, elevated ESR and CRP, and thrombocytosis. On imaging you see bilateral peripheral opacities
Chronic eosinophilic pneumonia
Difference from other etiologies (i.e. EGPA, ABPA, parasitic stuff) is peripheral (not central) involvement, association with ashtma but no systemic vasculitis symptoms, idiopathic (no triggers) and highly steroid responsvie
500
 "I got plenty of friends, I can name 3 right off the bat. __________"
"I got plenty of friends, I can name 3 right off the bat. __________"
The gang's all here