Conducting pathways
Anatomy and Physiology 1
Anatomy and Physiology 2
Tracheostomy Management 1
Tracheostomy Management 2
100
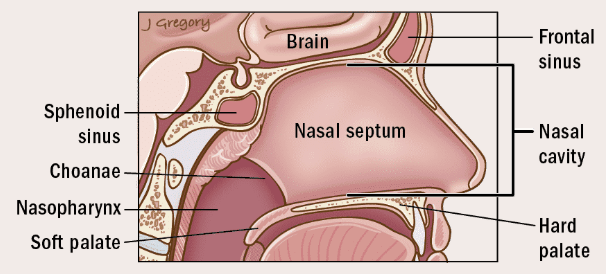
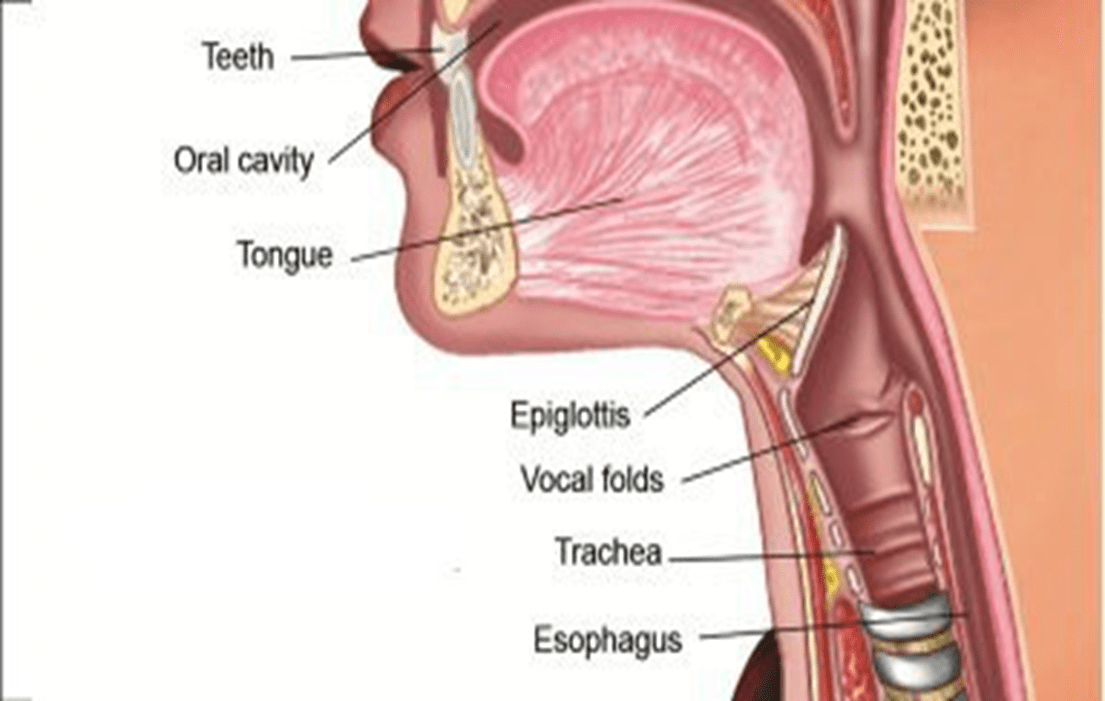
Air is first inspired through this structure.
Nasal Cavity
100
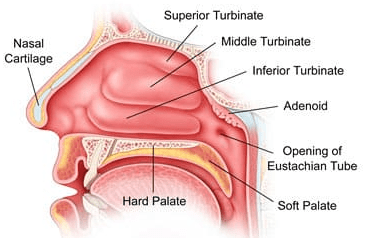
Found in the nasal cavity are structures or folds that are lined by a lot of blood vessels and mucous, when the air we breath hits these structures in our nasal cavity, the air spins and throws all the particulates in the air or pathogens into this mucous. These structures or folds are called
Turbinates
100
A Tracheostomy bypasses this part of our respiratory system
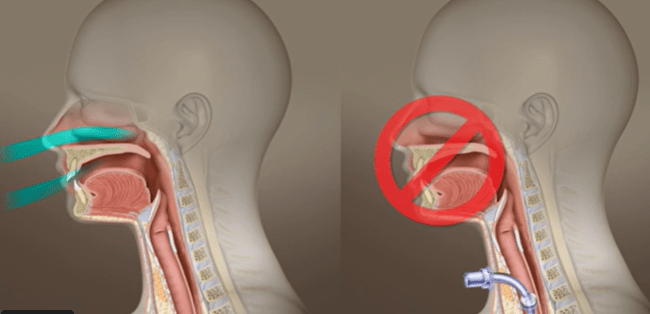
Upper Respiratory Tract
100
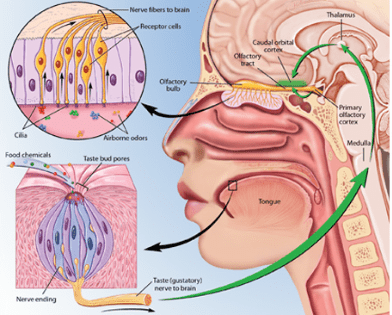
These two senses are impaired by a tracheostomy
Smell and Taste
100
An HME and/or the F&P Airvo provide this vital normal part of the conducting pathway
Humidification
200
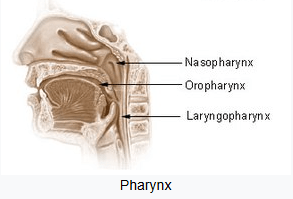
There are 3 parts to this structure within the Upper Respiratory Tract
Pharynx Nasopharynx, Oropharynx, Laryngopharynx
200
These structures in the lungs play a crucial role in respiratory health, acting as tiny, hair-like structures that line the airways. Their main function is to trap and move particles and pathogens out of the airways, helping to prevent infections and maintain clear air passages.
Cillia
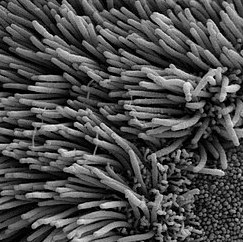
This movement, often compared to a wave, efficiently propels mucus loaded with dust, bacteria, and other foreign particles upward toward the throat, where it can be swallowed or expelled.
200
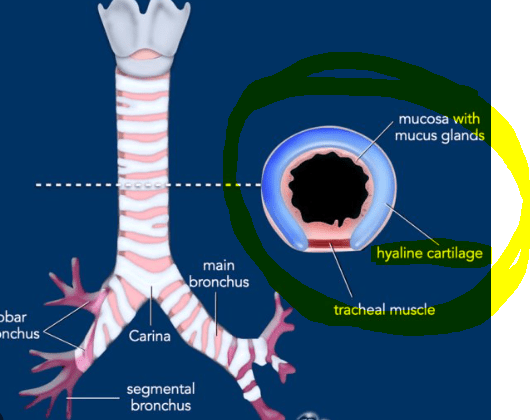
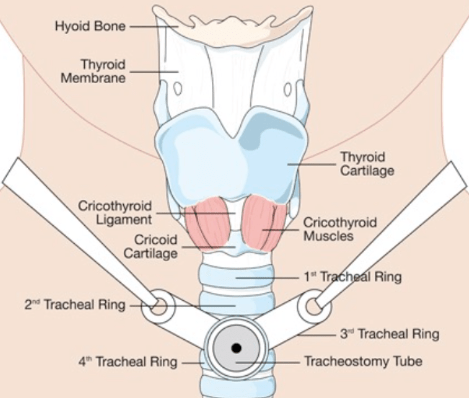
This part of our anatomy keeps our tracheal airways strong and open, like a straw to facilitate air movement for gas exchange
Cartilage
200
A Tracheostomy is typically placed approximately 2.5cm below this anatomical structure
Larynx
200
Used to check the cuff pressure on the Tracheostomy
Cuff Manometer
Ideal range is 20-30cmH20

300
The Larynx is the last part of the conducting pathway within the upper respiratory tract, this structure comes next...
Trachea
300
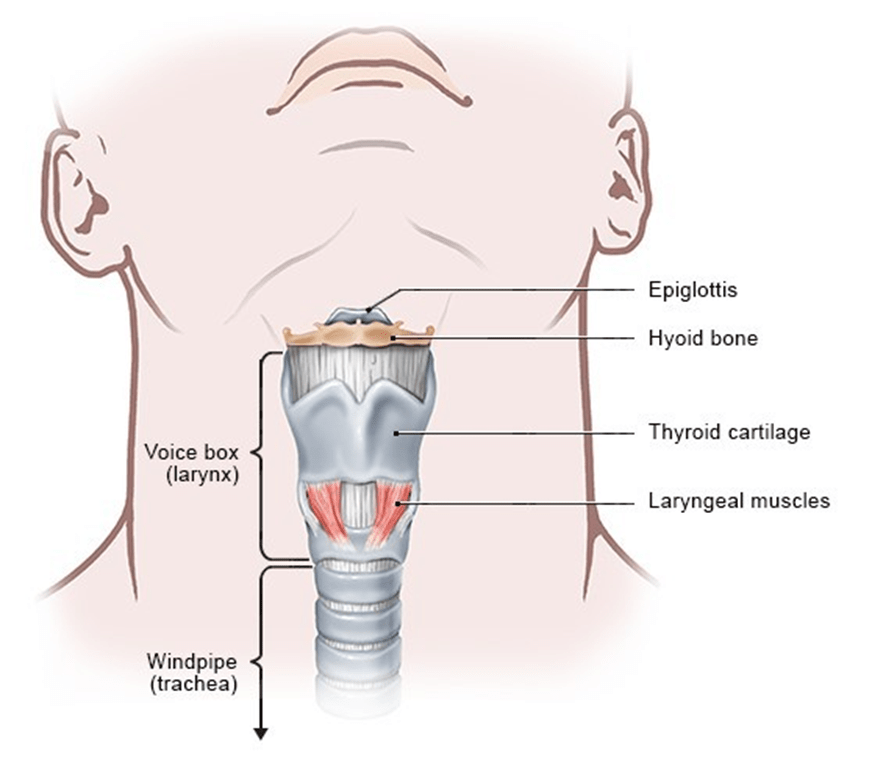
This structure is also known as our voice box
larynx
300
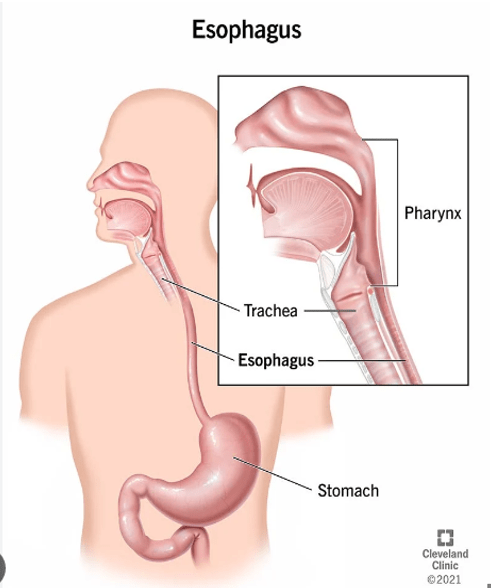
Carrys food and liquid from the mouth to the stomach via the pharynx (throat)
Esophagus
300
Must be checked and CHANGED at the start of each shift
Inner Cannula

300
This is only performed when clinically indicated for a tracheostomy patient
Suctioning
400
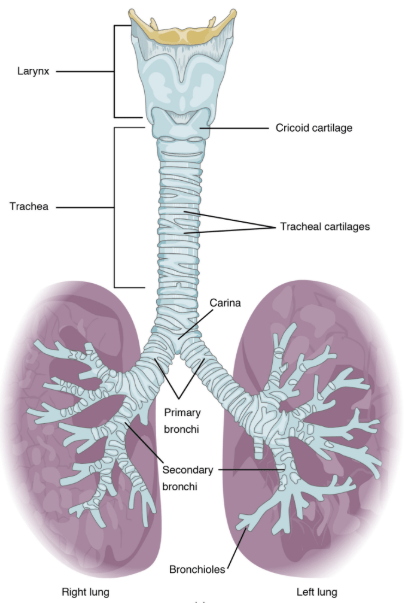
In the lower respiratory tract the Trachea splits and bifurcates into the left and Right main
Bronchi
400
This structure is like a small moveable lid, it helps us to swallow, and prevents food and drink from entering the lungs
Epiglotis
400
There is more of this structure in our lower airways, it plays an important role in breathing, helping the airways relax and constrict, or open and close for gas exchange.
Muscle
400
Important to be adequate prior to suctioning
Oxygenation
400
Structural piece of the Tracheostomy that is checked at the start of the shift, decreasing the risk of aspiration of secretions
Cuff
500
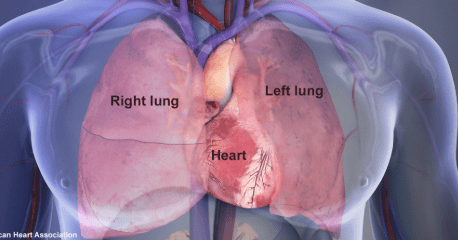
Bronchi branch about 23 times to be the right upper middle and lower lobes on the left side we have 2 lobes, this makes way for our
Heart
500
If the patient was to aspirate, the clinical structure most likely to facilitate this is the
The right main bronchi
Wider and more upright
500
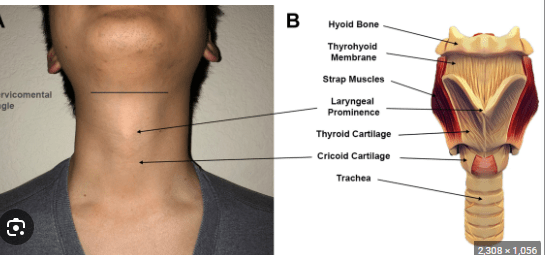
The adams apple is present in both males and females, what we see externally is clinically referred to as
Laryngeal Prominence
500
Inserting a suction catheter through a tracheostomy tube until resistance is met at this structure to remove secretions from the airway due to ineffective clearance
Carina
500
Maintaining the cuff pressure between 22-28mmHg is important to prevent these (name two)
- Reduced blood flow
- Tracheoesophageal fistula
- Tracheal Stenosis
- Tissue Damage/Necrosis
- Difficulty swallowing