Ventilator Initiation
Initial Settings
Ventilator Optimization
Pharmacology
Condition Specific Stabilization
100
What is the most important feature to consider when selecting a ventilator?
Clinician familiarity
100
The initial minute ventilation target for an adult patient receiving mechanical ventilation is approximately _________.
100 ml/kg/min
100
What is the calculation for driving pressure?
Plateau-total PEEP
100
You are preparing to intubate a patient and the RN tells you the patient's recent potassium was 6.1. What neuromuscular blocking agent would you recommend?
Rocuronium
100
A patient is intubated for status asthmaticus. When selecting a sedative agent, this medication may be considered due to additional respiratory effects beyond sedation.
Ketamine
200
Name 3 advantages of A/C-PC
Variable flow
Plateau pressure controlled
Sustained inspiratory pressure may result in more alveolar recruitment
Improved gas distribution
Lower PIP compared to VC w/ square wave form
200
If initiating a patient in PC, what initial inspiratory pressure should be set?
Range of 10-15 cm H2O above PEEP
200
Two patients have a plateau pressure of 28 cm H2O. Patient A has a PEEP of 5 and patient B has a PEEP of 15. Which has the lower driving pressure?
Patient B 28-15 = 13
Patient A 28-5 = 23
200
Name the reversal agents for:
-Rocuronium
-Benzodiazepines
-Opioids
-Rocuronium: Sugammadex
-Benzodiazepines: Flumazenil
-Opioids: Naloxone
200
Describe 3 ways severe metabolic acidosis contributes to hemodynamic instability.
•Reduction of left ventricular contractility (decreased stroke volume)
•Increased likelihood of cardiac arrhythmias
•Arterial vasodilation
•Decreased responsiveness to vasopressor medications
300
A patient with ARDS is placed on a mode designed to maintain alveolar recruitment by spending the majority of time at a high pressure with brief releases for ventilation. Identify the mode.
APRV
300
Which of the following ventilator settings would be MOST appropriate for a 5'5" female patient with ARDS?
a. PRVC 460, R-12, +8, 100%
b. VC 340, R-16, +8, 100%
c. SIMV-VC 340, R-16, +8, 100%
d. PRVC 400 R-16, +8, 100%
b. VC 340, R-16, +8, 100%
300
You increase PEEP from +8 to +12. Plateau pressure does not increase and oxygenation improves. What likely happened?
Lung recruitment?
300
A 58-year-old male with a BMI of 48 kg/m² presents with worsening shortness of breath and stridor. He has a history of head and neck cancer with a known upper airway mass. He is awake but becoming increasingly fatigued. Current assessment:
SpO₂ 92% on NRB, RR 32 breaths/min, Accessory muscle use present, Able to answer questions appropriately
Which of the following airway management strategies is MOST appropriate for this patient?
a. Perform RSI with induction agent and neuromuscular blockade followed by immediate intubation
b. Attempt NIV to avoid invasive airway placement
c. Perform awake fiberoptic intubation
d. Administer a paralytic first to improve visualization during intubation
c. Perform awake fiberoptic intubation
300
A patient with renal failure is intubated for respiratory failure. Assessment shows:
- pH 7.12
- PaCO₂ 25
- HCO₃ 8
- Na 140
- Cl 105
Calculate the anion gap and identify if it is increased, decreased, or normal. Should bicarbonate be given?
140 - (105+8) = 27
Elevated anion gap
No, bicarbonate should not be administered. Correct the cause of high anion gap acidosis
400
A sedated and paralyzed patient is receiving mechanical ventilation. The patient is making no spontaneous effort and every breath is initiated by the ventilator. What type of ventilation is occurring?
Controlled ventilation
400
Which of the following ventilator settings would be MOST appropriate for a 6'0" male patient intubated for a stroke?
a. PC 15/+5, R-12, 100% (exhaled Vt: 475 mL)
b. PC 25/+5 R-12, 100% (exhaled Vt: 624 mL)
c. PC 15/+5 R-16, 100% (exhaled Vt: 475 mL)
d. PC 18/+5 R-12, 100% (exhaled Vt: 550 mL)
c. PC 15/+5 R-16, 100% (exhaled Vt: 475 mL)
400
What is the patient's driving pressure based on the image below?
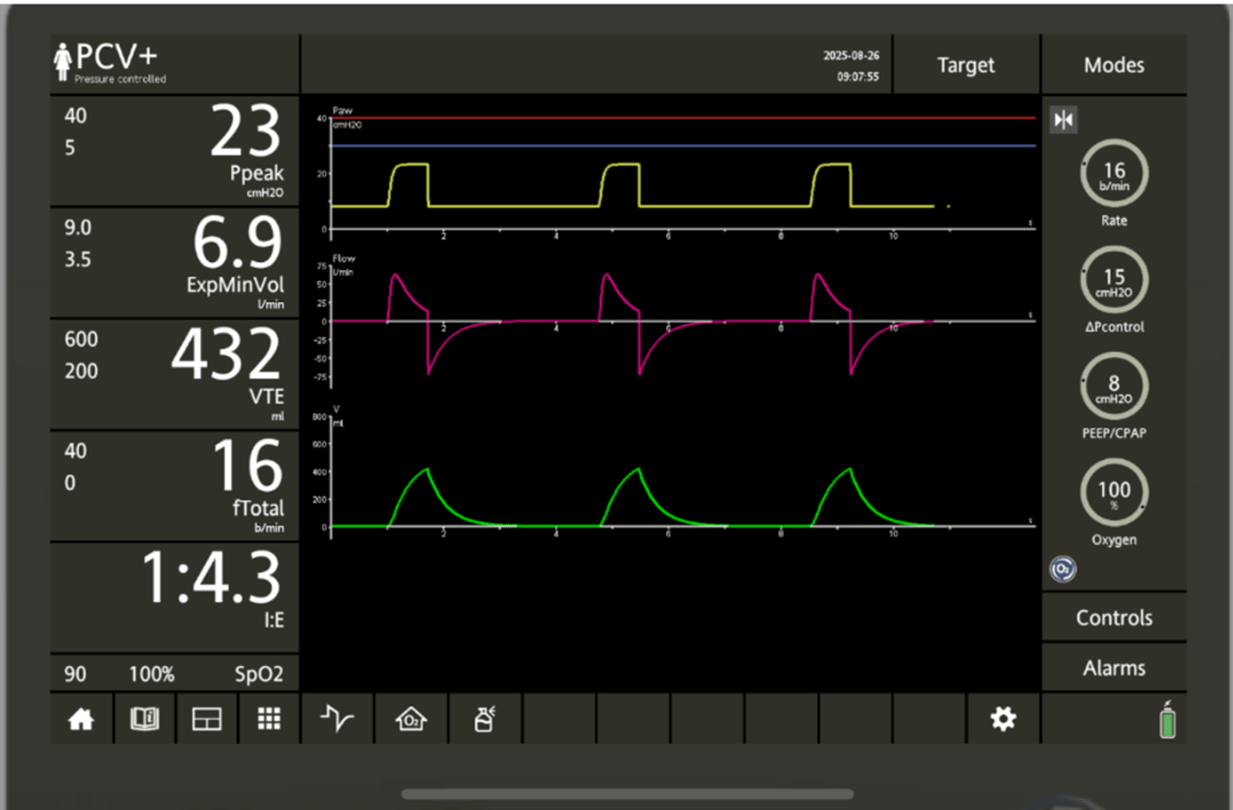
Need a plateau pressure
< 15 because inspiratory flow is not equilibrating
400
A 72-year-old male with pneumonia requires intubation due to worsening respiratory failure. Prior to intubation, assessment shows:
BP: 80/47 (58), HR: 115, RR: 28, SpO2 90% on nonrebreather
Which induction agent would be MOST appropriate for this patient during RSI?
Etomidate: hemodynamically neutral
Avoid propofol here
400
A patient presents with renal failure and pulmonary edema:
- pH 7.18
- PaCO₂ 28 mmHg
- HCO₃ 10 mEq/L
- K⁺ 6.5 mEq/L
- Creatinine 6.8 mg/dL
- CXR: bilateral pulmonary edema
What therapy should be considered to correct the underlying problem?
Dialysis
500
Your patient is in PC 18/+8. Their tidal volume decreases from 450 to 250 mL. Give 3 possible causes.
Decreased compliance
Increased resistance
Decreased patient effort
500
A 5'8" male patient is admitted with septic shock. His vitals are as follows:
HR-115, RR- 36, BP- 110/56, SpO2 - 98% on nonrebreather
ABG: 7.14/20/159/7
Which of the following initial ventilator settings would be MOST appropriate?
a. VC 410, R-16, +8, 100%
b. VC 550 R-14, +8, 100%
c. VC 410 R-20, +5 100%
d. VC 410, R-28, +5, 100%
d. VC 410, R-28, +5, 100%
500
You are performing a PEEP titration on your patient in VC. Which PEEP would you leave the patient on? Is your driving pressure goal met? If not, what ventilator adjustments could you make?
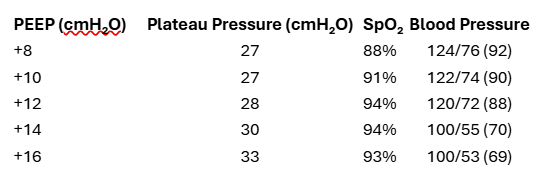
+12
At +14 BP was decreased 20%
Driving pressure 28-12 = 16, goal not met
Decrease tidal volume and increase RR to compensate
500
Your patient was recently intubated with Etomidate and Rocuronium and placed VC 320/16/+8/100%. Your vital signs are below, what would you recommend?
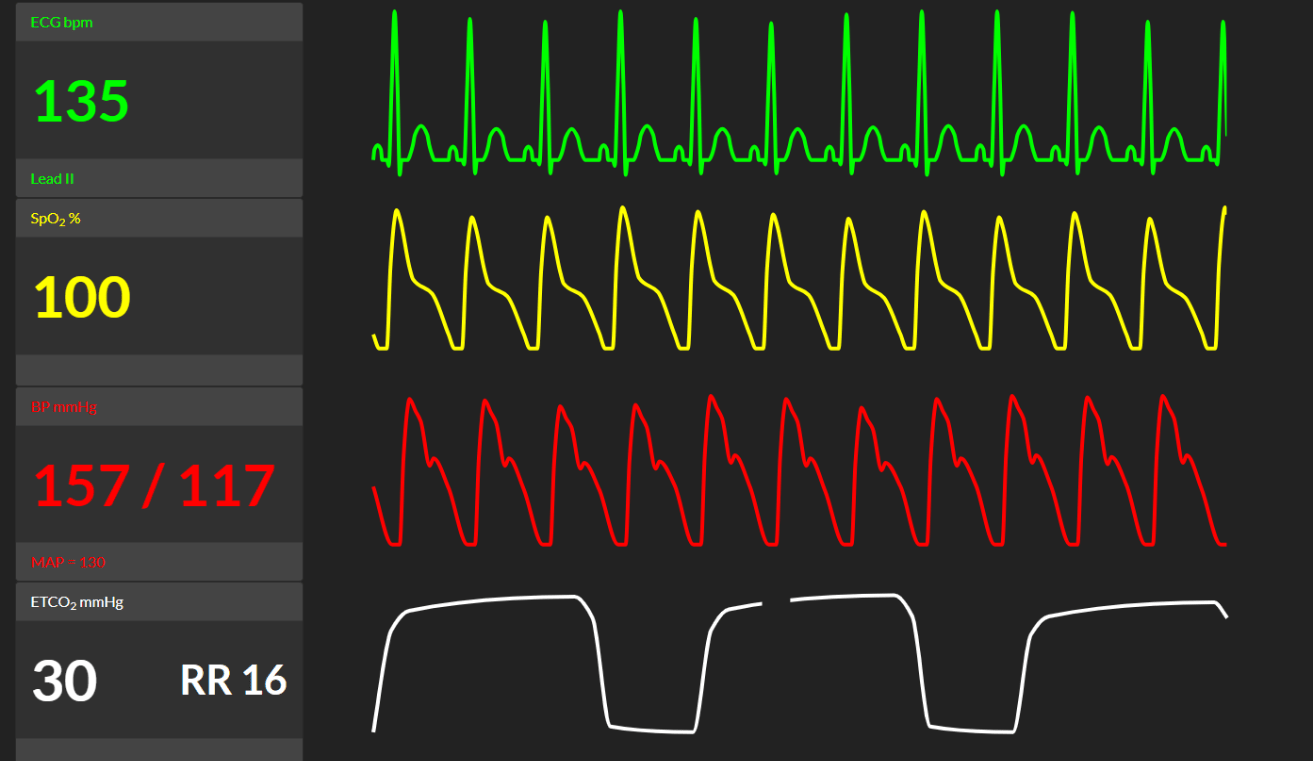
Start sedation, patient is paralyzed and not sedated
Etomidate 3 to 12 minute duration
Rocuronium 30 to 60 minutes duration
500
A patient with a traumatic brain injury is intubated for airway protection.
Current assessment:
- ICP: 28 mmHg
- BP: 130/75
- Vent: VC VT 480 mL, RR 12, PEEP +5, FiO₂ 40%
- ABG: 7.28 / 55 / 95 / 25
Why could the current ventilator strategy worsen the patient’s neurologic status?
Hypoventilation causing CO2 retention
Increased PaCO2: cerebral vasodilation, increased cerebral blood volume, increased ICP