Risky business ;)
Cut it out
~*MeLaNoMa*~
Wildcards
100
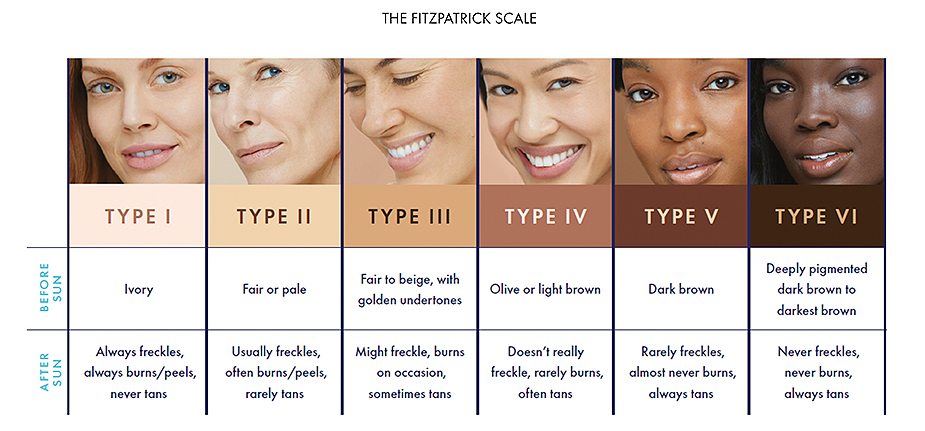
"I always get a sunburn!" It's my Fitzpatrick type

What is Fitzpatrick Type 1?
100
A 56-year-old man comes to the office because of a lesion on the tip of his nose. He has a 10-year history of coronary artery disease, skin cancers, excisions of the face, and poorly controlled type 2 diabetes mellitus. He has smoked one pack of cigarettes daily for the past 30 years. Medications include 81 mg of aspirin daily. Physical examination shows a 1-cm nodule with irregular borders. Examination of a specimen obtained on biopsy shows morpheaform basal cell carcinoma. Which of the following is the most appropriate next step in management?
Moh's Micrographic Surgery
Morpheaform basal cell carcinoma is notorious for having "finger-like" extensions that are not always apparent on gross visual examination and can only be appreciated histologically. The morpheaform subtype of basal cell carcinomas tends to have a higher recurrence rate when simply excised. Mohs micrographic surgery is a technique that uses tangential excisions and frozen section pathology, which more accurately assess the margins of excision. Mohs micrographic surgery may also help minimize the extent of resection. Mohs micrographic surgery is particularly useful in morpheaform basal cell carcinoma, where obtaining negative surgical margins is critical to minimizing the risk of recurrence.
100
ABCDEs of melanoma

100
patients with a history of ____ or _____ have a risk of developing _____ (this lesion) 
1. what is radiation? What is lymphedema?
2. what is angiosarcoma
Angiosarcoma is a rare (2% of all soft-tissue sarcomas) but highly aggressive tumor that is most commonly found in the face and scalp in older Caucasian men. Fifty percent of all cutaneous angiosarcomas are found in the head and neck, and they are also commonly found in the breast and extremities, particularly in patients with a history of lymphedema or radiation therapy. It appears initially as a purple plaque which is often confused with a bruise or cellulitis, which can delay diagnosis. It is frequently multifocal, and local recurrences are common, so wide local excision is recommended, frequently combined with radiation therapy.
200
xeroderma pigmentosum is a autosomal recessive disorder characterized by mutation of this
nucleotide excision repair
Xeroderma pigmentosum results from a mutation in nucleotide excision repair. The nucleotide excision repair system is capable of removing ultraviolet-induced damage to DNA, such as pyrimidine dimers and pyrimidines 6-4 pyrimidones
200
this lesion (measuring 3 cm) should be taken with this margin
What is 6 mm? (6-10 mm)
low risk -> 4mm: well-differentiated tumors smaller than 2 cm in diameter
high risk -> 6mm: larger than 2 cm, invasive to fat, or in high-risk locations (i.e., central face, ears, scalp, genitalia, hands, feet)
200
the cells that form tumors in melanoma are derived from this embryologic cell origin
What are neural crest cells?
200
A 79-year-old man has a rapidly growing lesion on the left side of his forehead. Physical examination shows a 2-cm, raised, fungating lesion of the left temple with intact facial nerve function and no lymphadenopathy. Examination of a specimen obtained on biopsy is suspicious for squamous cell carcinoma. Four weeks later, the lesion has disappeared, leaving a small circular scar. Excision is performed, and pathologic study shows no evidence of malignancy. Which of the following is the most likely diagnosis?
keratoacanthoma
The most likely diagnosis is keratoacanthoma, a low-grade malignancy that resembles squamous cell carcinoma both clinically and pathologically. The most common natural course of the disease is that of rapid growth followed by spontaneous regression over several months, which is not seen in squamous cell carcinoma.
300
UVA radiation is more/less abundant and more/less carcinogenic than UVB
UVA radiation is more/less abundant and more/less carcinogenic than UVB
300
Your patient is a 91 year old male with his fifth occurence of squamous cell carcinoma. Punch biopsies show 7 new lesions on his ear, nose, cheek, forehead, and scalp all consistent with squamous cell carcinoma. Patient would be best treated with this therapy
topical 5-fluorouracil
300
this subtype of melanoma tends to be slow-growing
Lentigo maligna is melanoma in situ that primarily occurs in elderly patients with a history of extensive sun exposure. It represents 4 to 15% of all melanomas and is slow-growing in a radial phase, but can progress to lentigo maligna melanoma with invasion and metastatic potential.
Surgical resection remains the standard of care for treatment of lentigo maligna
300
HIV+ patient presents with this rash. This is the most likely diagnosis
Kaposi sarcoma is an interesting soft tissue tumor occurring in several distinct populations with a variety of presentations and courses. In its most well-known form, Kaposi sarcoma occurs in patients with immunosuppression, such as those with acquired immunodeficiency syndrome (AIDs) or those undergoing immunosuppression due to an organ transplant. Initially described in 1872 by Moritz Kaposi, an Austro-Hungarian dermatologist in 5 patients with the multifocal disease,[1] human herpesvirus/Kaposi sarcoma herpesvirus (HHV-8) was discovered as a causative agent of Kaposi sarcoma as the AIDS epidemic progressed in the 1980s.[2] Four clinical forms emerged.
400
Use of this topical agent in addition to use of sunscreen can suppress skin carcinogenesis
Vitamin-A derivatives
Topical and systemic retinoids are effective prophylactics and therapeutics for several types of non-melanoma skin cancers, including BCC, SCC, Kaposi Sarcoma, cutaneous T-cell lymphomas, and more
400
this lesion has a 95% chance of negative margins if cut out using this size margin
What is 3 mm?
Many studies have had various observations as to the least margin required to cure a basal cell carcinoma. Almost all are retrospective, and conclusions have ranged greatly. Most articles recommend a 4-mm margin. However, in aesthetically sensitive areas like the eyelid, knowing the minimum margin of resection is crucial. Of course, Mohs micrographic surgery is an alternative, but it is not always feasible because of cost, availability, and the difficulty in coordinating two physicians’ schedules. A recent meta-analysis of the literature concluded that for basal cell carcinomas 2 cm or less, a 3-mm margin is sufficient to achieve at least a 95% chance of cure.
400
this phenomenon is known as 
Hutchison sign
Acral-lentiginous melanoma is the rarest in Caucasians but accounts for greater than 30% of all melanomas that occur in dark-skinned individuals.
nail beds. In the subungual presentation, they commonly cause a longitudinal line in the nail plate known as Hutchinson sign.
400
this rapidly growing lesion presents as a raised, indurated, irregularly shaped violaceous plaque and arises from mesenchymal cells in the dermis
dermatofibrosarcoma protuberans (DFSP)
It accounts for less than 0.1% of all malignant neoplasms and approximately 1% of all soft-tissue sarcomas, but is the most common type of cutaneous sarcoma. It is a malignant mesenchymal tumor that arises in the dermis and is characterized by latency in its initial detection, slow infiltrative growth, and local recurrence if not adequately treated. Distant metastasis is rare and generally occurs as a late sequela after repeated local recurrences. DFSP is most commonly found on the trunk followed by the proximal extremities, and rarely in the head and neck. These tumors have irregular shapes, frequent finger-like extensions, and an infiltrating growth pattern extending beyond clinical margins that result in incomplete removal and a propensity for local recurrence. Treatment primarily consists of wide surgical excision to include margins of 2 to 3 cm beyond the clinical tumor border if possible. Mohs micrographic surgery has been used with good outcomes in aesthetically sensitive areas such as the head and neck where tissue sparing is important. Reconstruction with tissue rearrangement or flaps should be performed after negative margins are confirmed. Most recurrences occur within 3 years of the primary excision, and close follow-up is indicated.
Conventional chemotherapy is rarely used. Radiation therapy is used as an adjunct to surgery for close or positive margins in areas where adequate wide resection alone may result in major cosmetic or functional deficits. Molecular targeted therapy such as imatinib mesylate (Gleevec) is indicated for unresectable, recurrent, or metastatic DFSP. Sentinel node biopsy is not indicated in the treatment for DFSP.
500
Chemical sunscreens absorb UV (usually UVB) radiation with the most common sunscreen ingredient being ______, ______, and ____. (must get 1) Physical sunscreens work by reflecting UV radiation and producing a protective barrier. They are usually opaque and include agents such as _____ and _______ (must get 1)
Chemical sunscreens absorb UV (usually UVB) radiation with the most common sunscreen ingredient being para-aminobenzoic acid (PABA), benzophenones, and cinnamates. Physical sunscreens work by reflecting UV radiation and producing a protective barrier. They are usually opaque and include agents such as zinc oxide and titanium dioxide.
500
A 60-year-old man comes to the office because of a 2-cm pigmented lesion on the right lower back (shown) that has enlarged progressively for 3 years. No lymph nodes are palpable. Examination of a specimen obtained on punch biopsy shows a Clark Level IV malignant melanoma with a Breslow thickness of 1.2 mm and ulceration. Which of the following is the most appropriate management?
Preoperative lymphoscintigraphy, sentinel lymph node biopsy, and excision with 2-cm margins

A melanoma 1.2 mm in thickness on the lower back would best be excised with 2-cm margins and a concurrent sentinel lymph node biopsy. Although a few studies cite the adequacy of a 1-cm margin for tumors less than 2 mm in thickness, a punch biopsy was performed in the scenario described, and the final pathology of the complete lesion could show a thicker lesion. In a location where there is sufficient tissue, a 2-cm margin is more appropriate for a lesion that is over 1 mm in thickness. Most authors cite resection margins of 5 mm for melanoma in situ, 1 cm for melanoma less than 0.8 mm, and 2 cm for melanoma between 0.8 and 4 mm.
500
These are the components of the melanoma pathology report (must get 5 out of 8)
1. Breslow thickness
2. Ulceration status (present or absent)
3. Dermal mitotic rate (#/mm2 )
4. Assess deep and peripheral margin status
5. Microsatellitosis (present or absent)
6. Pure desmoplasia if present
7. Lymphovascular/ angiolymphatic invasion
8. Neurotropism/perineural invasion
500
this rare tumor _____, requires treatment with ____ and _____
1. Merkel Cell carcinoma
2. wide local excision & radiation
Merkel cell carcinoma is a rare tumor that usually consists of smooth, painless, indurated, solitary dermal nodules approximately 2 to 4 mm in size. It occurs more frequently in patients older than age 65 years. Merkel cell carcinoma appears most often at sun-exposed sites on white skin; 50% occur on the head and neck, and 40% on the trunk. Merkel cell carcinoma is an aggressive tumor; metastases to regional lymph nodes are noted on initial diagnosis in 12 to 15% of patients. Regional metastasis eventually occurs in one half to two thirds of patients. Local recurrence following primary excision develops in 24 to 44% of patients. Time from diagnosis of the primary tumor to clinically apparent regional nodal metastases is approximately 7 to 8 months. Distant metastases occur ultimately in one third of patients; in order of frequency, metastases occur in the lymph, liver, bone, brain, lung, and skin. The mean time from diagnosis to systemic involvement is 18 months, with death occurring 6 months later. The 5-year survival rate has been reported as 30 to 64%. Two thirds or more of patients with local or regionally recurrent disease ultimately die. Surgical excision is the treatment of choice for primary tumors. The prevailing opinion regarding Merkel cell cancers is that they should be excised with margins similar to those for melanoma.
Sentinel lymph node biopsy is used in clinically node-negative patients with Merkel cell carcinoma.
Radiation should be considered for all patients with Merkel cell carcinoma, as it is radiosensitive. Injection of 5-fluorouracil and administration of interferon have never been shown to be effective in Merkel cell treatment.
In Merkel cell carcinoma, tumor width dictates surgical excision, not tumor depth of invasion (as in melanoma).