Bugging Out
Shots Fired
Immunology
Rejects & Regrets
Cellebrities
100
A 6-year-old boy presents with a sore throat and fever. Exam shows tonsillar exudates and tender anterior cervical lymphadenopathy.
Which organism is most likely responsible?
What is streptococcus pyogenes
100
A clinician says a patient’s post vaccination antibody titer is expected to fall over time and periodic doses will be needed to maintain protection. This pattern best fits this broad category of vaccines.
What are inactivated vaccines?
Inactivated vaccines produce weaker responses, require multiple doses, and often need periodic boosts.
100
Triggered by antigen exposure in the lymph node, this process involves rapid, random mutations specifically in the variable region of antibody genes to increase the affinity for a given epitope.
What is Somatic Hypermutation? Occurs in the dark zone of the germinal center.
100
This immunologic mechanism involves recipient IgG antibodies binding donor endothelium, activating complement, and causing thrombosis.
Type II hypersensitivity reaction. - Hyperacute Rejection
Pre-existing recipient antibodies
react to donor antigen (type II
hypersensitivity reaction), activate
complement
100
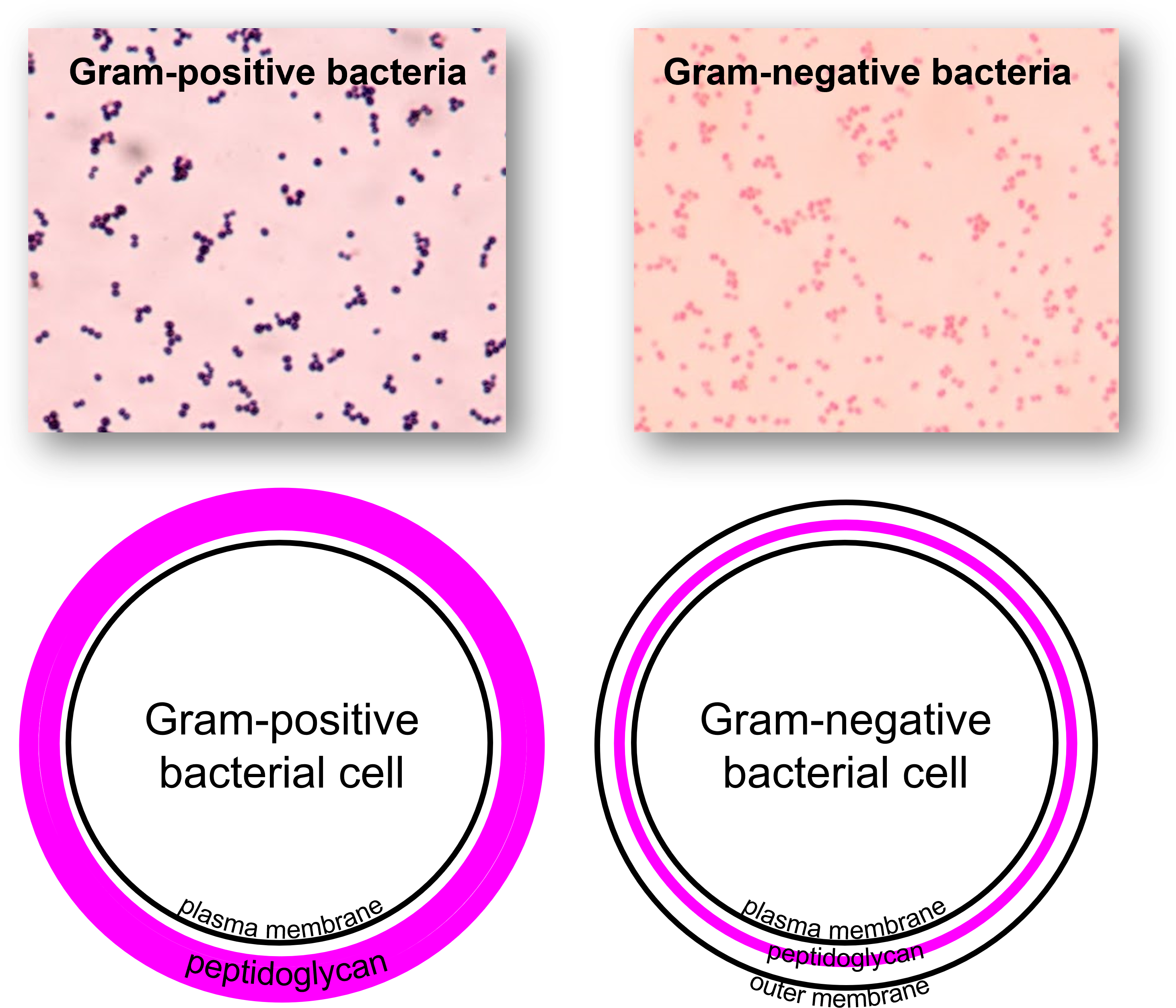
How will gram (-) vs gram (+) bacteria appear under a normal gram stain?

- Gram-positive bacteria (Gram +)
- Appearance: Purple / blue
- Reason:
- Thick peptidoglycan traps crystal violet–iodine complex
- Does NOT wash out with alcohol
- Examples:
- Staph, Strep, Clostridium
- Gram-negative bacteria (Gram −)
- Appearance: Pink / red
- Reason:
- Thin peptidoglycan loses crystal violet during alcohol wash
- Then takes up safranin counterstain
- Examples:
- E. coli, Pseudomonas, Neisseria

200
A child presents with fever, conjunctivitis, cough, and a rash that began on the face and spread downward.
What is the most likely organism?
What is measles virus
200
A healthy 5-year-old develops fever and a mild rash one week after routine immunization. His mother is told this can occur because limited replication of the immunizing agent took place after administration
What is a live attenuated vaccine?
These vaccines mimic natural infection more closely, which is why they often produce strong immunity, but they can also produce mild, self-limited symptoms resembling a very small version of the disease.
200
This enzyme complex is responsible for converting molecular oxygen into superoxide radicals; its deficiency results in recurrent abscesses from catalase-positive organisms like S. aureus and Aspergillus.
What is NADPH Oxidase? (The condition is Chronic Granulomatous Disease)
200
A patient improves after treatment with tacrolimus. This drug works by inhibiting this transcription factor pathway.
calcineurin → NFAT inhibition → ↓ IL-2 transcription?
200
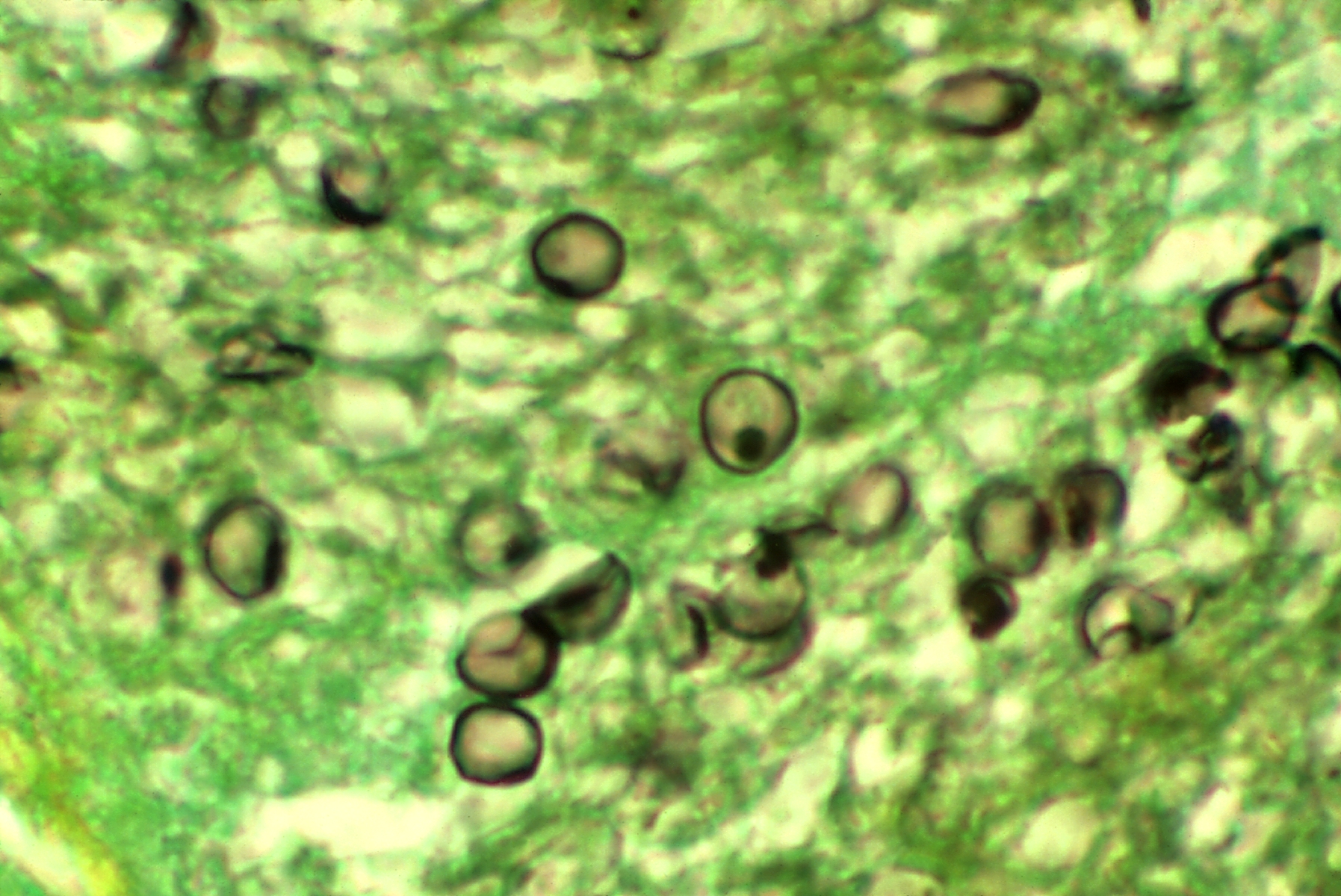
A 23-year-old man comes to the physician for a 1-week history of orange discoloration of his urine. Urinalysis shows 1+ blood. He has had no recent illnesses he can recall. Four months ago he went traveling through western Africa for two weeks with a group of friends. What organism is causing these symptoms? Bonus: Tx?

- Key clues
- Hematuria (orange urine + blood)
- Travel to Africa
- Image shows:
- Egg with terminal spine
- Diagnosis
- Schistosoma haematobium
- Why this fits
- Lives in:
- Venous plexus of bladder
- Causes:
- Hematuria
- Urinary symptoms
- Egg:
- Terminal spine (classic)
- Lives in:
- Treatment
- Praziquantel
300
A patient from the Ohio River Valley presents with fever and cough. Imaging shows calcified granulomas. Biopsy reveals macrophages filled with small intracellular yeasts.
What is the most likely pathogen?
What is histoplasma capsulatum
300
A medical student receives a booster after stepping on a nail. The immunizing agent protects by generating neutralizing IgG against a bacterial product that prevents release of inhibitory neurotransmitters from Renshaw cells.
What is the tetanus toxoid vaccine?
Clostridium tetani causes disease through its toxin, not through invasive spread of the organism itself. The vaccine therefore uses an inactivated toxin (toxoid) that is no longer toxic but is still antigenic.
The immune system then makes neutralizing Immunoglobulin G (IgG, Immunoglobulin G) antibodies against the toxin. Those antibodies prevent the toxin from acting on neurons.
300
To prevent the premature binding of self-antigens while in the endoplasmic reticulum, this specific protein occupies the MHC Class II peptide-binding groove until it is degraded in the acidified endosome.
What is the Invariant Chain? (The remaining fragment in known as CLIP)
300
This pathologic process involves smooth muscle proliferation and narrowing of graft vessels.
What is graft vasculopathy (intimal thickening)? - Chronic Rejection.
CD4+ T cells respond to recipient
APCs presenting donor peptides,
including allogeneic MHC
Both cellular and humoral components
(type II and IV hypersensitivity
reactions)
300
- A 34-year-old homeless man presents to the emergency department with a 2-week history of worsening fever and nonproductive cough. He has a history of HIV infection but has been noncompliant with antiretroviral therapy. His CD4+ T-cell count is 160 cells/mm³. Chest imaging shows diffuse bilateral interstitial infiltrates. Organism? Tx?
- Pneumocystis jirovecii
- Tx
- Trimethoprim-sulfamethoxazole
- Why (NBME logic)
- CD4 < 200 → think opportunistic infection
- Subacute fever + dry cough + hypoxemia + diffuse interstitial infiltrates → classic for Pneumocystis jirovecii pneumonia (PCP)
- BAL with cysts → confirms PCP
- First-line treatment = TMP-SMX
- Yes — this is exactly why HIV patients receive TMP-SMX prophylaxis
- It is primarily to prevent Pneumocystis jirovecii pneumonia (PCP), which is a high-risk, life-threatening opportunistic infection when CD4 < 200
400
A 35-year-old presents with abdominal pain. Physical examination reveals a palpable, non-tender mass in the right upper quadrant. Imaging shows a large hepatic cyst containing multiple daughter cysts.
What pathogen is most likely responsible?
What is echinococcus granulosus
At risk of anaphylaxis if it ruptures!
400
An infant receives one form of passive immune protection from maternal secretions that helps protect their gut lining.
What is Immunoglobulin A (IgA, Immunoglobulin A)?
The passive immune protection in maternal secretions, especially breast milk and colostrum, is mainly Immunoglobulin A (IgA, Immunoglobulin A) in its secretory form.
400
This specific transcription factor is required for the development of regulatory T-cells; a deficiency leads to a severe X-linked syndrome involving enteropathy, polyendocrinopathy, and dermatitis.
What is FOXP3 (The condition is IPEX syndrome)
400
This drug inhibits mTOR and blocks IL-2 signaling, preventing T-cell proliferation.
What is sirolimus?
400
- A 55-year-old man with poorly controlled type 2 diabetes mellitus is brought to the emergency department with fever and progressive swelling around his left eye. On examination, there is periorbital edema and a black necrotic lesion on the nasal mucosa. Laboratory studies show hyperglycemia and metabolic acidosis. Histologic examination of a biopsy specimen from the affected tissue is shown. Which of the following is the most likely causative organism?

- Correct answer: Rhizopus species (mucormycosis)
- Step-by-step NBME reasoning
- Underlying condition
- Poorly controlled diabetes is the #1 classic risk factor for mucormycosis
- Clinical presentation clues
- Facial pain + sinus symptoms
- Periorbital swelling → spread from sinuses to orbit
- Black necrotic eschar on nasal mucosa
- This is EXTREMELY high-yield
- Histology (what seals the diagnosis)
- Broad, ribbon-like hyphae
- Nonseptate
- 90° branching
- → this pattern = mucormycosis (Rhizopus/Mucor)
- Underlying condition
- Why the answer is specifically Rhizopus
- NBME uses Rhizopus as the representative organism of mucormycosis
500
A 19-year-old college freshman is brought in with confusion and fever. His roommate says several students recently had a “flu-like illness.” Exam shows petechiae on the trunk and extremities.
What is the most likely organism?
What is neisseria meningitis
BONUS: what are the other common causes of meningitis? (1 per age group)
500
The reason one pneumococcal formulation performs poorly in infancy is not failure of antigen recognition, but predominance of this type of B-cell response.
What is a T-cell-independent response?
A polysaccharide antigen can bind directly to the B-cell receptor (BCR, B-cell receptor) and activate B cells without much helper T-cell involvement.
BONUS - This linked component allows a polysaccharide vaccine to recruit helper T cells.
500
A mutation in the gene encoding this specific protein leads to a failure of negative selection in the thymic medulla, resulting in a triad of hypoparathyroidism, adrenal insufficiency, and chronic mucocutaneous candidiasis.
What is AIRE?
500
A post-transplant patient develops rash and diarrhea. Another patient with a kidney transplant develops graft failure due to lymphocyte infiltration. This key distinction explains the difference:
What is GVHD = graft attacks host; rejection = host attacks graft?
500
A 66-year-old man comes to the physician for a 2-day history of high fever and severe leg pain. Physical examination shows darkening of the skin of the leg and crepitus. He has a 30-year history of type II diabetes mellitus and hypertension managed with multiple medications. Vitals are: temperature 103°F, HR 80, RR 20, BP 150/90. A gram stain of the causal organism is shown.
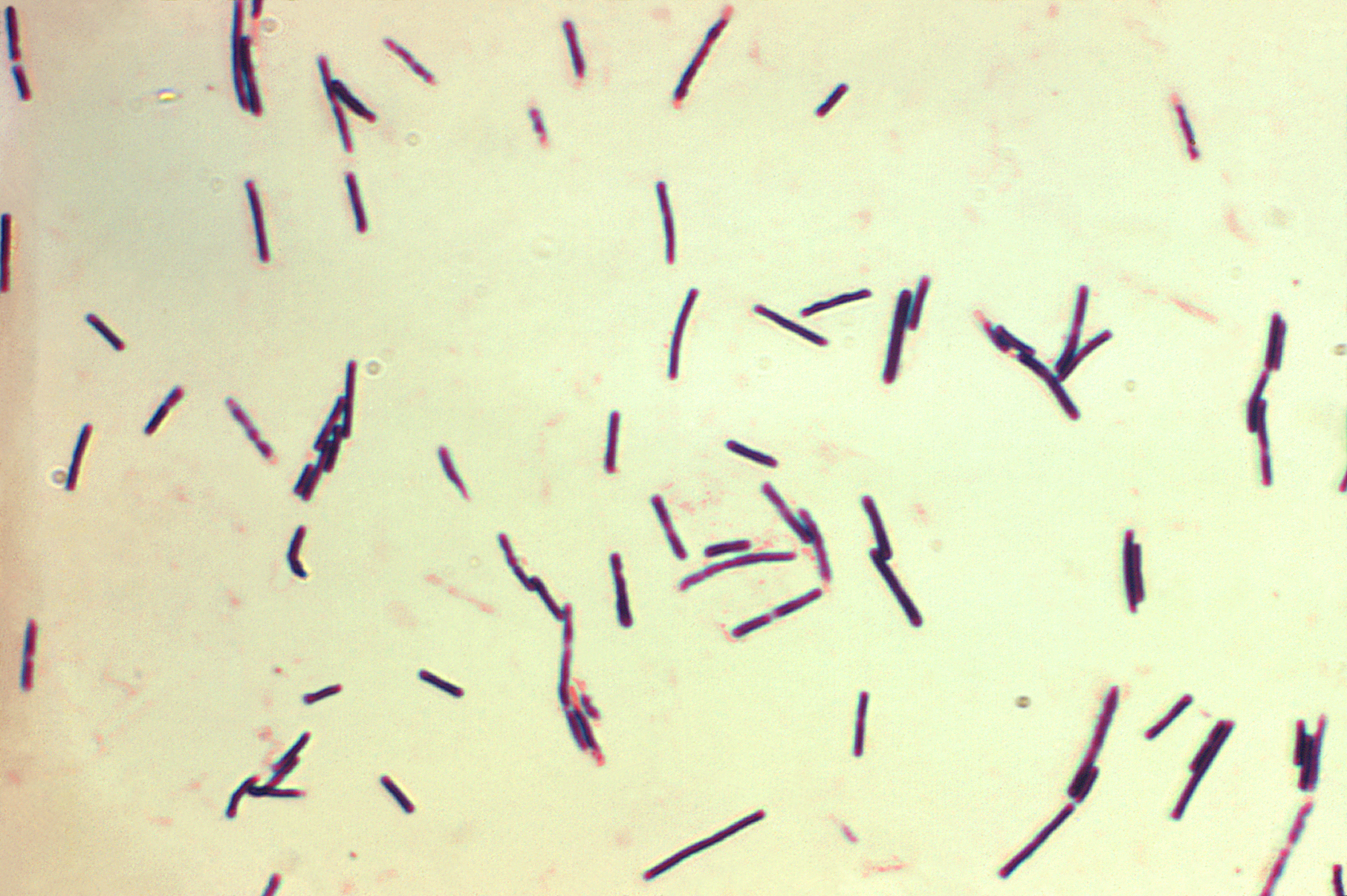
Which virulence factor is the most likely explanation for this patient’s findings?
A. Coagulase
B. Exotoxin A
C. Lipid A
D. Lipoteichoic acid
Clostridium perfringens
α-toxin = phospholipase C (lecithinase)
- Gram-positive anaerobic rod
- α-toxin = phospholipase C (lecithinase)
- Breaks down cell membrane phospholipids
- → myonecrosis
- → hemolysis
- → gas formation
- Why others are wrong
- Coagulase
- Staph aureus → abscesses, not gas gangrene
- Exotoxin A
- Pseudomonas → inhibits EF-2
- Lipid A
- Gram-negative endotoxin → septic shock
- Lipoteichoic acid
- Gram-positive cell wall component, not toxin causing necrosis
- Coagulase